Abstract
The biomechanical etiology of the so-called idiopathic scoliosis [Adolescent Idiopathic Scoliosis (AIS)] has been the subject of the author’s research since 1984. The problem was presented on many orthopedics congresses, symposia and also in “competent groups” who are specialized in the problem of “idiopathic scoliosis” in SOSORT and IRSSD meetings. I have given lectures on this matter in SOSORT Meetings in Athens and Wiesbaden (Germany), in IRSSD Meetings in Athens, Genth (Belgium), Liverpool, Poznan (Poland) and in SICOT Congresses in Havana (Cuba), Istanbul (Turkey), Kołobrzeg (Poland), and Marrakesh (Morocco) [1–28].
Keywords
Scoliosis, Etiology, Symptoms, New classification, Therapy.
Material
In the years 1984 – 2018, more than 2500 patients with scoliosis have been observed and treated (80%). In 20 % there were older patients coming because of spinal pain. Older people with pain problems were in the second or third group of the new Lublin classification of scoliosis (see next chapter – classification).
Classification
“The model of hip movements” (T. Karski – described in 2006) explains the new classification of scoliosis. When movements of hips are equal, scoliosis never develops. There is no biomechanical pathological influence acting on the spine. The growth of spine is proper.
When movements of hips are asymmetrical – there is an input to develop scoliosis in the three groups and four types.
Scoliosis “S” 1st etiopathological group (epg) [Fig. 1]- double curve. Stiff spine (3D). Rib hump on the right side of the thorax. Connection with gait and standing „at ease’ on the right leg.
-
- Scoliosis “C” 2nd/A epg [Fig. 2] – one curve – lumbar left convex. Spine flexible (1D or 2D). Connection with standing „at ease’ on the right leg only.
- Scoliosis “S” 2nd/B epg [Fig. 2] – two curves, (2D or 3D). Connection with standing ‘at ease’ on right leg and additionally with laxity of joints or / and harmful previous exercises.
In these second 2a and 2b types of scoliosis – the spine is flexible.
- Scoliosis “I” 3rd epg [Fig. 3]. Deformity has the form of a stiff spine, (2D or 3D). No curves or small ones. The cause is gait only. Such “spine deformity” was till 2004 never included / classified as “scoliosis”.
The Questions and the Authors Answers to the Problem of Scoliosis [1–28].
The etiology of idiopathic scoliosis was unsolved through many centuries and many questions are discussed in the world till now.
In research of etiology of the so-called idiopathic scoliosis everybody who will answer the question: what is “the etiology?” – must answer the all below presented questions about scoliosis or even more. Answering only some questions is not enough and is not the answer for cardinal question “what is the etiology”.
The Questions are following:
- The etiology – of course – the subject of whole discussion?
- Why girls have more frequent scoliosis?
- Why do we mostly observe the lumbar left convex curve?
- Why do we mostly observe the thoracic right convex curve?
- When there is one curve scoliosis and when there are two curves scoliosis?
- Why the rib hump (gibbous costalis) is on the right side?
- When does scoliosis start to develop – at what age?
- What kind of classification is proper? What is the patient’s type of scoliosis?
- Why there is a rapid progression of scoliosis in the period of accelerated growth during the childhood?
- Which type of scoliosis progresses?
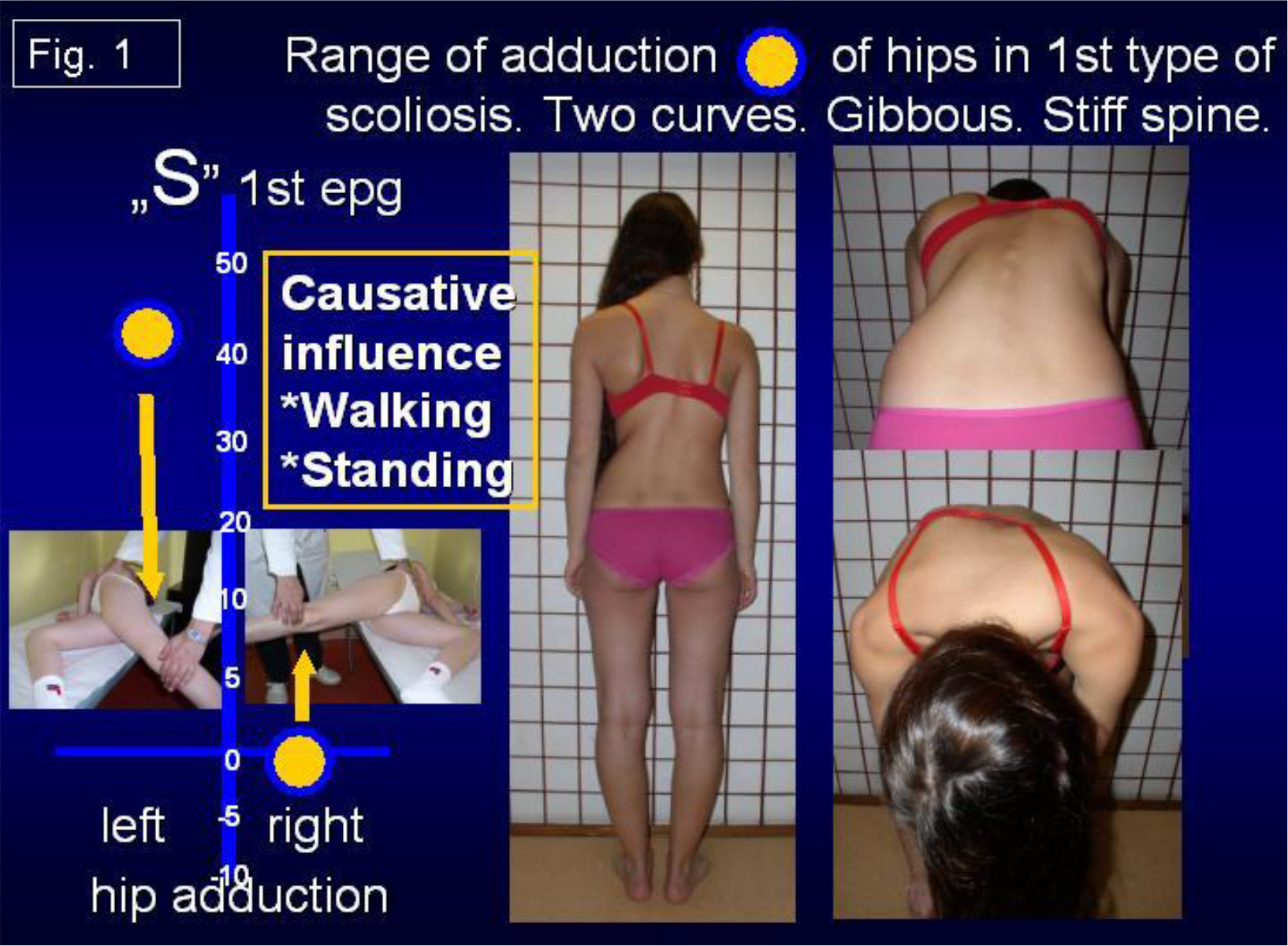
Figure 1. Range of adduction of hips in 1st type of scoliosis. Two curves. Gibbous. Stiff spine. Causative influence: walking & standing.
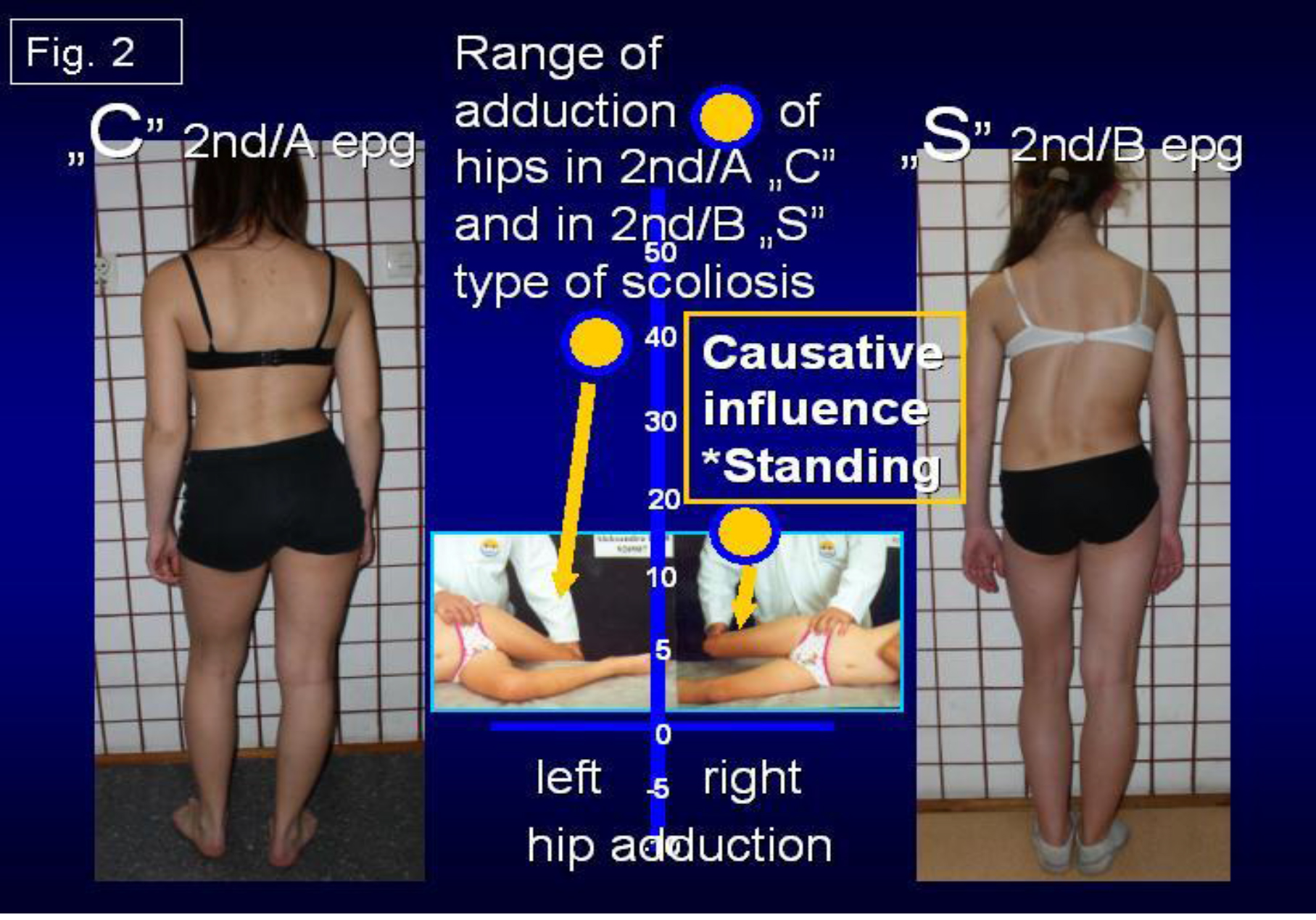
Figure 2. Range of adduction of hips in 2nd/A „C” and in 2nd/B „S” type of scoliosis. Causative influence: standing.
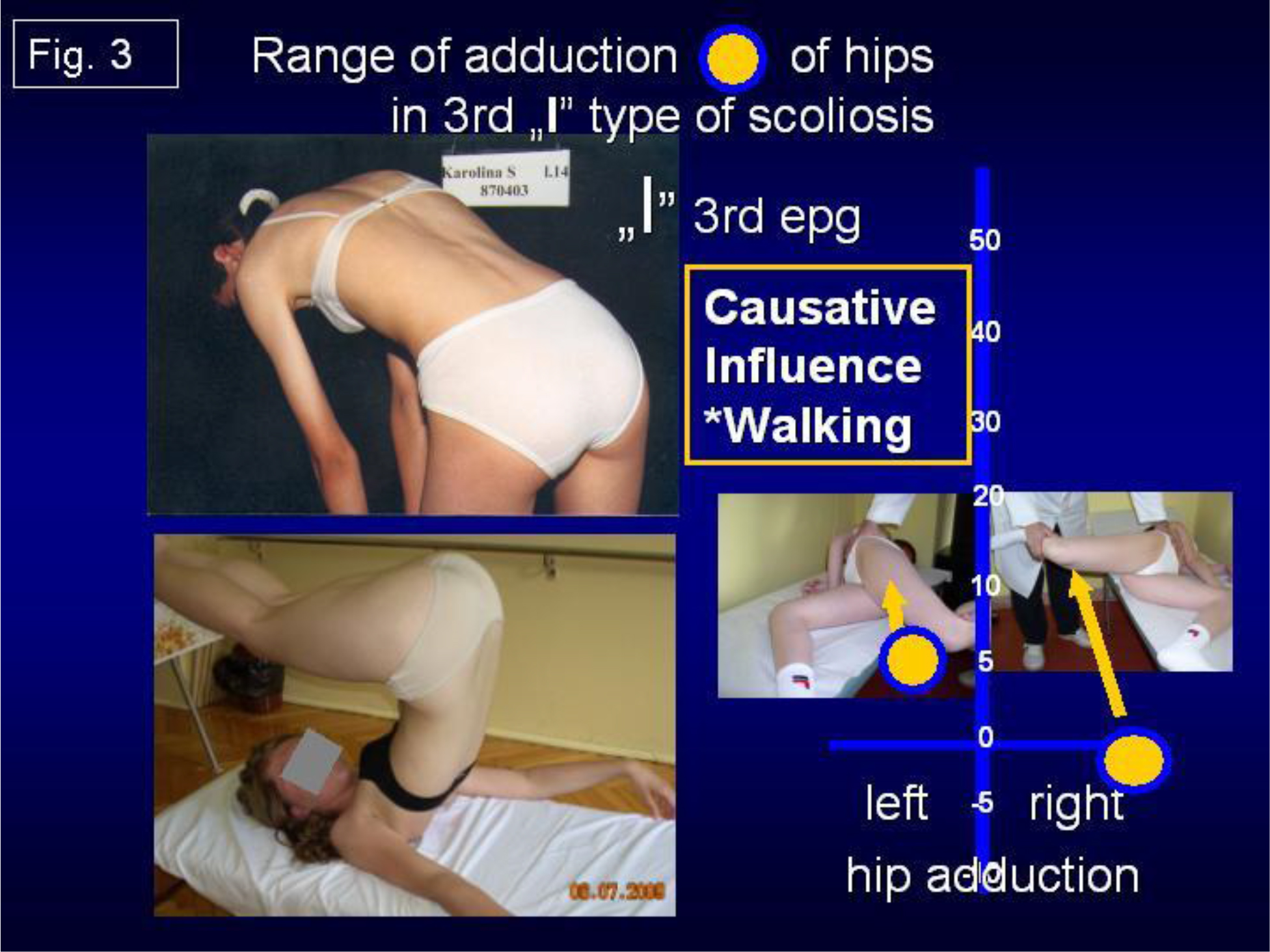
Figure 3. Range of adduction of hips in 3rd „I” type of scoliosis. Causative influence: walking.
- Which type of scoliosis does not progress?
- Why blind children do not have scoliosis?
- Is there any influence of CNS in development of scoliosis? Direct influences? Indirect influences?
- What kind of therapy – conservative or operative should be used in treatment?
- Are extension and strengthening exercises correct?
- What kinds of rehabilitation exercises should be applied?
- Is corset (orthopedic devices) treatment proper – yes? no?
- Is causative prophylaxis possible?
My Answers and Comments:
For all these questions the only answer is “biomechanical etiology of so-called scoliosis”. This idea of etiology is presented in my lectures and articles in years 1995 – 2019 – also in Web Site www.ortopedia.karski.lublin.pl
I have given lectures during the IRSSD Meetings – in 2002 in Athens, in 2006 in Ghent, in 2008 in Liverpool, in 2012 in Poznań, in two SOSORT Congresses and on many others Congresses – e.g. during SICOT in Cairo, in Havana, in Istanbul, next in Germany, in Hungary, in Czech Republic, in Slovak Republic, in Hong Kong, in China / Beijing, in Finland e.g. .
The only answer to all the questions informs about the etiology of scoliosis! If somebody answers only partially to the question about etiology – the etiology presented by him is not correct.
Here, I present my answer to all the questions on the basis of “biomechanical influences”:
- The Etiology is biomechanical. Connected with asymmetry of anatomy of body of children (already in newborns and babies) and next connected with the asymmetry of movements in many joints – but – especially important – asymmetry in range of movement of hips. All these asymmetries are connected with “The Seven Contractures Syndrome” (“Siebener [Kontrakturen] Syndrom” – according to Prof. Hans Mau) [see Literature] or The Syndrome of Contractures and Deformities [SofCD, 2006] – T. Karski).
Because of these “asymmetries” – it is *asymmetry of loading during gait, *asymmetry of time of standing on left / right leg – more on the right (!), *asymmetry in development and growth of spine, *in result scoliosis in three ethiopathological groups & four types.
- Why girls have more frequent scoliosis? Answer SofCD – appears mostly in girls. Girls are more sensible for forces during pregnancy (especially if the fetus has not enough space in uterus) and next such children / girls more frequently suffer from “Syndrome of Contractures and Deformities”.
- Why lumbar left convex curve? Answer: The SofCD is mostly “left sided” (90 % – 95 % of pregnancies – Prof. Jan Oleszczuk / Lublin and all gynecologists). Permanent standing on the right leg – is due “contracture” more stable (!) but makes lumbar left convex scoliosis / curve. A child told me – I stand on the right leg – because it is more comfortable, more stable, more easy, it doesn’t tire me, I like to stand on the right leg e.g.
- Why thoracic scoliosis / curve is right convex? Answer: The SofCD is mostly “left sided”. 90 % – 95 % of pregnancies are “left sided pregnancies” – Literature: Prof. Jan Oleszczuk / Lublin and all gynecologists on the world. Permanent standing on the right leg (this leg due “contracture” is more stable) makes lumbar left convex scoliosis / curve and secondary right convex thoracic curve in 2nd / B ethiopathological group (epg). Some cases in “S” 2nd / B epg scoliosis are “kifoscoliosis / kiphoscoliosis”. Important remark: in I-epg group both curves – lumbar left convex and thoracic right convex develop at the same time – look at the following points.
- Why there can be one curve or two curves in scoliosis? The answer is – one curve scoliosis “C” lumbar left convex deformity is in 2nd / A epg group connected with standing ‘at ease’ on the right leg. The scoliosis in form of “S” is in 1st epg group – spine is stiff and also formed in “S” form in 2nd / B epg group – spine is flexible. These both types of scoliosis are double curve deformities.
- Why the rib hump (gibbous costalis) is on the right side? The answer: The SofCD is mostly “left sided”. 90 % – 95% of pregnancies are “left sided pregnancies” – Literature: Prof. Jan Oleszczuk / Lublin and all gynecologists on the world. In “S” 1st epg group permanent standing on the right leg – this leg due to a “contracture” is more stable, it triggers the lumbar left convex scoliosis and secondary right convex scoliosis. Due to walking and permanent rotation distortion in inter-vertebral joints a rib hump develops on the right side. Important remark: such rotation distortion appears because of compensatory movement while the adduction and internal rotation movement in right the hip in 1st epg group of scoliosis is maximally limited. Rotation deformity and stiffness develop primarily. This rotation deformity develops in three stages: a/ flat back, b/ disappearance of processi spinosi, c/ in some cases lordotic deformity in thoracic part of spine. Some cases in “S” 1st epg scoliosis are “lordoscoliosis”.
- When scoliosis starts to develop – in which year of the life of the child ? Every type of scoliosis starts to develop when the child starts “standing” and “walking” – at the age of two.
The “S” scoliosis in 1st epg can be observed very early – at the age of 4 – 6. The “C” 2nd/A epg scoliosis and “S” 2/B epg can be spotted at the age of 10 – 12. First it is only physiological deviation movement of the spine and – later “a fixed deformation” in the form of scoliosis.
- What kind of classification is proper? There are three groups and four types of scoliosis. All groups in this “new classification” are connected with “the model of hips movements” (T. Karski, 2006):
1st epg –“S” scoliosis with stiffness of spine – some types of scoliosis in 1st epg are “lordotic scoliosis” – connection with gait and with permanent standing ‘at ease’ on right leg, 2nd/A “C” scoliosis – connection with permanent standing ‘ at ease’ on right leg, 2nd/B “S” scoliosis – connection with permanent standing ‘at ease’ on right leg – plus laxity of joints and wrong exercises (!). Some types of scoliosis in 2nd / B epg are “kypho-scoliosis”) 3rd epg “I” scoliosis – small curves or none, small gibbous or none – only stiffness of spine. The 3rd epg scoliosis is only connected with gait / walking.
Here I repeat – every type of scoliosis starts developing when the child starts standing and walking.
- Why is there a rapid progression of scoliosis in the period of accelerated growth of the child? Answer: bones grow – even 10 cm – 15 cm per year in some children. Contracted soft tissue in the region of the right hip does not grow and its influence is bigger(!). Especially in children whose legs growth faster than the trunk.
- Which type of scoliosis progresses? The progression is in the “S” 1st epg scoliosis
- Which type of scoliosis does not progress? The 2nd/A epg, 2nd/B epg and 3rd epg type scoliosis are without progression. In scoliosis 3rd epg – patients notice the problem in the adult age – because of pain. Young people have problems doing sports – but almost nobody believes that the problem is connected with the stiffness of the spine in special type of scoliosis.
- Why blind children do not have scoliosis? The gait of blind children protects from scoliosis – they walk without lifting legs, instead every step is very careful. The walking model is totally different than in healthy children.
- Is there any influence of CNS in the development of scoliosis? Direct influences? Indirect influences? Yes – there are only indirect influences in children with Minimal Brain Dysfunction (MBD) or with Attention Deficit Hyperactivity Disorder (ADHA) – [according author – MBD and ADHD are equal]:
- extension contracture of the trunk in small children – because of spastic (semi spastic) contracture of trunk extensors,
- anterior tilt of pelvis – because of spastic (semi spastic) contracture of m. rectus both sides,
- “laxity” of joints – because of changed properties of collagen. In some cases laxity is the cause of progression of scoliosis. According to Prof. Harald Thom – 10 % of children with CP or MBD are with laxity (with Prof. Thom personal contacts in Heidelberg 1972 – 1973 during authors DAAD scholarship time and next in Rummelsberg / Nürnberg).
- What kind of therapy – conservative or operative should be applied in treatment? Answer: only conservative – in my material from years 1995 – 2009, only 13 % children need surgery and there were children previously treated by wrong, incorrect exercises / methods. In years 2010 – 2019 the number of children needing surgery in my material is maximally low – 3 % or less.
- Are extension exercises correct? [Fig. 4a, 4b, 4c] No – such exercises are wrong – they cause “iatrogenic deformity” – bigger curves, bigger rib hump, stiffer spine. Wrong exercises can change the direction of curves. They are the cause of extra – additional curves. They can be the cause of “three curves scoliosis”. Every doctor in every country should stop such wrong exercises.
- What kinds of rehabilitation exercises should be applied? [Fig. 5a, 5b, 5c, 6a, 6b] Only – stretching exercises – giving symmetry of movements and next symmetry of growth and development of pelvis and spine. In the first place – we should receive / restore the “full symmetry of all movement of hips”, next symmetry of “function of trunk muscles”. For spine there are very important “bending / flexions exercises” even in very small children (age 3 – 4 years) such passive exercises are possible. When the child has full, symmetrical movements of both hips – it is no more asymmetry of loading of body left / right side during walking and no more “permanent standing ‘at ease’ on right leg” – but “symmetrical time of standing left / right leg”. In such situation scoliosis never develops.

Figure 4. 4a, 4b, 4c. Example of incorrect therapy. Karolina 16 y. old. Four years incorrect therapy by improper / wrong exercises (2012 – 2016) in Kxyz and in Zxyz (Poland). As a result – iatrogenic big deformity. Consultation in Lublin on 1st June 2016. „S” scoliosis in 1st epg (etiopathological group). Two curves. Gibbous on the right side of thorax. Stiffness. Length of corpus 53 cm, of legs 92 cm. Start with new therapy. In such cases achieving good results is impossible. All children need causal prophylaxis.

Figure 5. 5a, 5b, 5c, 5d. Example of correct therapy. Child Natalia in age 10 years. No 060712. Double curve scoliosis in 2nd/B type of deformity. Additionally rickets. Figure 5c show in Adams test slight rotation deformity. Axis of spine after therapy normal. Treatment in Lublin three years. Important – standing ‘at ease’ on the left leg (Fig 5d). See next figures with X-ray.
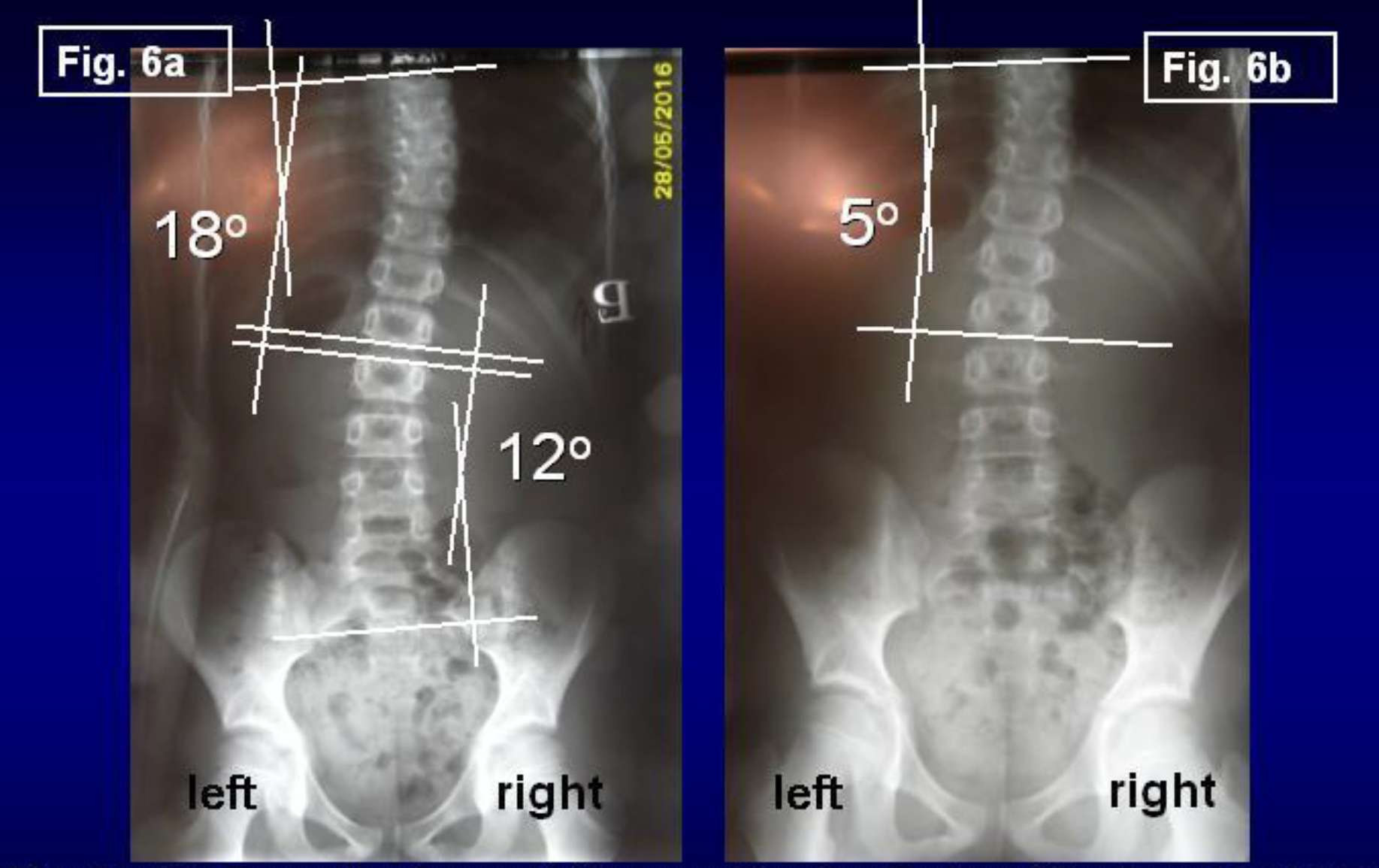
Figure 6. 6a, 6b. Example of correct therapy. Karolina P. Age 10y. Born 12.07.2006. No 060712. Fig. 6a – before treatment in Lublin. Fig. 6b – after 3y. of new treatment. In therapy: 1/ standing ‘at ease’ on the left leg, 2/ every day flexion exercises forwards, left and right direction, 3/ sleeping in embryo position, 4/ karate.
- Corset (orthopedic devices) treatment – yes ? no ? I use the corset in 20 % of children in “S” 1st epg scoliosis and in 5% – 10% of children in “S” 2nd / B epg scoliosis.
- Is causative prophylaxis possible? Yes – and should be introduced in all countries. First, doctors should inform parents / patients that all previous methods of treatment – for example extensions, “muscles strengthening exercises” were incorrect and harmful. They only cause bigger curves and make the spine stiffer. Because of this, orthopedic surgeons in the past used to speak about “Natural History of Scoliosis” to explain to parents and treated children bad results of therapy.
Exercises leading to symmetry of movements and symmetry of function of hips and spine are important in prophylaxis and therapy. All exercises removing flexion contractures of both hips, removing abduction contracture or only “too small range of adduction” of the right hip, removing external rotation contracture of right hip and extension contracture of whole spine belong to these methods. We should remember that the rigidity of spine is very often the first step on the way to scoliosis in “S” 1st epg group of scoliosis.
Flexion exercises for spine should be introduced already in small children at the age of 3 – 5. Also is very important to inform parents or patients about position of standing – all children endangered with scoliosis should stand ‘at ease’ only on the left leg. Standing ‘at ease’ on the right leg is permanent and after some years (important – cumulative time of standing) plays a very important role in etiology of scoliosis. Standing on the left leg is not permanent and does not leading to scoliosis.
Conclusion
- In all years of observations (T. Karski, 1984 – 2018), the biomechanical etiology of the so-called idiopathic scoliosis was confirmed.
- Development of scoliosis and the types of spine deformity are connected with pathological “model of hips movements” (T. Karski, 2006) and function – “standing ‘at ease’ on the right leg” and “walking”.
- Restricted range of movements in the right hip is connected with the “Syndrome of Contractures and Deformities” according Prof. Hans Mau.
- Every type of scoliosis starts to develop at the age of 2–3.
- There are three groups and four types of scoliosis:
“S” scoliosis 1st epg, 3D. Causative influence: standing and gait,
- “C” scoliosis 2nd / A epg, 1D. Causative influence: standing.
- “S” scoliosis 2nd / B epg, 1D or 2D. Causative influence: standing, plus, – laxity of joints and/or incorrect exercises in previous therapy.
- “I” scoliosis 3rd epg, 2D or 3D. Clinically only stiffness of the spine. Causative influence: gait. The clinical symptom of this deformity is – sport problems at a young age and “permanent pain” in adults.
The proper therapy of scoliosis – are only stretching exercises help to obtain full movements of the right hip, the proper position of the pelvis and full movement of the spine.
The causal prophylaxis of scoliosis is possible and should be introduced in every country.
The rules in prophylaxis – are – standing ‘at ease’ on the left leg, sitting relax, sleeping in embryo position, active participation in sport – especially in karate, taekwondo, aikido and other similarly.
Acknowledgement: I would like to express my many thanks to Honorata Menet for correction of the article.
References
- Burwell G, Dangerfield PH, Lowe T, Margulies J. Spine (2000) Etiology of Adolescent Idiopathic Scoliosis: Current Trends and Relevance to New Treatment Approaches 14: 324.
- Green NE, Griffin PP (1982) Hip dysplasia associated with abduction contracture of the contralateral hip. J Bone Joint Surg Am 64: 1273–1281. [crossref]
- Hensinger RN (1979) Congenital dislocation of the hip. Clin Symp 31: 1–31. [crossref]
- Howorth B (1977) The etiology of the congenital dislocation of the hip, Clin Orthop 29: 164–179.
- Karski T (2002) Etiology of the so-called “idiopathic scoliosis”. Biomechanical explanation of spine deformity. Two 272 groups of development of scoliosis. New rehabilitation treatment. Possibility of prophylactics, Studies in 273 Technology and Informatics Research into Spinal Deformities 91: 37–46.
- Karski T, Kalakucki J, Karski J (2006) “Syndrome of contractures” (according to Mau) with the abduction contracture of the right hip as causative factor for development of the so-called idiopathic scoliosis. Stud Health Technol Inform 123: 34–39. [crossref]
- Karski T (2010) Explanation of biomechanical etiology of the so-called idiopathic scoliosis (1995 – 2007). New 276 clinical and radiological classification” in”Pohybove Ustroji” [Locomotor System] vol. 17, 2010, No.1 + 2, pages: 277 26 – 42 (Czech Republic – 2010) 278.
- Karski T (2011) Biomechanical Etiology of The So-Called Idiopathic Scoliosis (1995 – 2007) – Connection with 279 “Syndrome of Contractures” – Fundamental Information for Paediatricians in Program of Early Prophylactics / 280 Journal of US-China Medical Science 8: 281
- Karski Tomasz (2010) Factores biomechanicos en la etiologia de las escoliosis dinominadas idiopaticas. Nueva 282 clasificacion. Nuevos test clinicos y nueavo tratamento conservador y profilaxis”, Cuestiones de Fisioterapia, Mayo- 283 Agosto 2010, volumen 39, Numero 2, paginas 85 – 152 [Cuest. Fisioter. 2010, 39 (2); 144 – 152] / Spain [2010] 284
- Karski Tomasz (2010) Biomechanical Etiology of the So-called Idiopathic Scoliosis (1995–2007). New Classification: 285 Three Groups, Four Sub-types. Connection with „Syndrome of Contractures”. Pan Arab J Orth Trauma 14: 287.
- Karski Tomasz (2013) Biomechanical Etiology of the So-called Idiopathic Scoliosis (1995 – 2007). Three Groups and 288 Four Types in the New Classification, Journal of Novel Physiotherapies, OMICS Publishing Group 289 6: 290.
- Karski Jacek, Tomasz Karski (2013) So-Called Idiopathic Scoliosis. Diagnosis. Tests Examples of Children Incorrect 291 Treated. New Therapy by Stretching Exercises and Results, Journal of Novel Physiotherapies, OMICS Publishing 292 Group, USA, 2013, 3–2, 9 pages 293.
- Karski Tomasz (2014) Biomechanical Aetiology of the So-Called Idiopathic Scoliosis. New Classification (1995 – 2007) in Connection with “Model of Hips Movements”. Pages 12. Global Journal of Medical Research H: Orthopedic and Musculoskeletal System 14.
- Karski Tomasz (2014) Biomechanical Etiology of the So-called Idiopathic Scoliosis (1995 – 2007) – Connection with„ Syndrome of Contractures” – Fundamental Information for Pediatricians in Program of Early Prophylactics. Surgical Science 5: 33–38.
- Karski Tomasz, Karski Jacek (2015) Syndrome of Contractures and Deformities” according to Prof. Hans Mau as Primary Cause of Hip, Neck, Shank and Spine Deformities in Babies, Youth and Adults American Research Journal of Medicine and Surgery 1.
- Karski Tomasz, Jacek Karski (2015) Biomechanical etiology of the so-called Idiopathic Scoliosis (1995 – 2007). Causative role of „gait” and „permanent standing ‘at ease’ pn the right leg”. New classification. Principles of new therapy and causal prophylaxis. Canadian Open Medical Science & Medicine Journal, Vol. 1: 1–16.
- Tomasz Karski, Jacek Karski (2016) Bóle krzyza – problem neurologiczno – ortopedyczny. Objawy. Przyczyny. Leczenie. Back pain – neurology-orthopedic problems. Clinic, causes, therapy and prophylaxis. Postepy Neurologii Praktycznej, Wydawnictwo Czelej. 4/2016, Str. 9 – 16.
- Karski Jacek, Karski Tomasz (2016) Imperfect hips” As a Problem at an Older Age. Early and Late Prophylactic Management before Arthrosis. Jacobs Journal of Physiotherapy and Exercises 015: 7.
- Karski Tomasz (2018) Biomechanical Aetiology of the So-called Adolescent Idiopathic Scoliosis (AIS). Lublin Classification (1995–2007). Causative Influences Connected with “Gait” and “Standing ‘at ease’ on the Right Leg”, Journal of Orthopaedics and Bone Research (USA), Scholarena, pages 10.
- Mau H (1979) Zur Ätiopathogenese von Skoliose, Hüftdysplasie und Schiefhals im Säuglinsalter. Zeitschrift f. 294 Orthop. 5, 601–5. 295.
- Mau H (1982) Die Atiopatogenese der Skoliose, Bücherei des Orthopäden, Band 33, Enke Verlag Stuttgart, 1 – 296 110 297.
- Mau Hans – personal information and letter.
- Normelly H (1985) Asymmetric rib growth as an aetiological factor in idiopathic scoliosis in adolescent girls, 298 Stockholm 1–103. 299.
- Stokes IAF (1999) Studies in Technology and Informatics, Research into Spinal Deformities 59: 1–385.
- Sevastik J, Diab K (1997) Studies in Technology and Informatics, Research into Spinal Deformities 37: 1–509. 301.
- Sevastik John – personal information.
- Thom Harald – personal information.
- www.ortopedia.karski.lublin.pl