DOI: 10.31038/IGOJ.2018108
Abstract
Aim: The aim of this study was to investigate the association between follicular fluid (FF) AMH and follicular fluid (FF) soluble receptor of Advanced Glycation End products (sRAGEs) in women with Polycystic Ovarian Syndrome (PCOS) regarding IVF outcome parameters.
Methods: FF AMH, serum AMH and FF sRAGEs were measured in 49 women undergoing IVF in the IVF Department of University Hospital of Alexandroupolis from December 2014 to May 2015. Women were divided in two groups, the PCOS women and the non PCOS women (Group A 38 non PCOS women and Group B 12 PCOS women). FF AMH, serum AMH and FF sRAGE values of Group A were compared to those of group B. The correlation of these values with IVF outcome parameters was investigated in both groups.
Results: We did not find a correlation among the factors studied (serum AMH, FF AMH and FF sRAGES). FF sRAGE levels were found to be higher in PCOS women (p-value <0,01). No correlation of FF sRAGE concentration and number of oocytes retrieved during IVF or number of embryos was noted in PCOS women. FF sRAGE levels were only found to be negatively correlated with the quality of the oocytes retrieved in non PCOS women (r= -0.484, p-value= 0.003). The higher the FF sRAGE concentration, the lower the quality of the oocytes was found to be. A negative correlation was also noted between FF sRAGE levels and BMI in non PCOS women (r= -0.401, p-value=0.014).
Conclusion: These findings support that FF sRAGEs could not be used combined with AMH measurements (serum and FF) to predict IVF outcome but could be used separately and only in non PCOS women.
Keywords
AMH, oxidative stress, sRAGEs, PCOS, ovarian reserve, IVF outcome
Introduction
Firstly described in 1935 by Stein Leventhal 1], Polycystic Ovary Syndrome (PCOS), is the most common endocrine disorder among reproductive-aged women and the main cause of female infertility due to anovulation, affecting the 19,9 % of Caucasian women under the Rotterdam criteria [2]. It is, therefore, understood that determining ovarian reserve- the quality and quantity of ovarian follicles at a given point in time and being able to predict total IVF outcome in women with PCOS is of great importance in Assisted Reproduction Technology (ART) [3].
Ovarian reserve markers
Up to date, many markers including FSH, estradiol, inhibin B, anti-Müllerian hormone (AMH), the antral follicle count (AFC), the ovarian volume (OVVOL) and the ovarian blood flow, have been studied and proposed as ovarian reserve markers [3].
Among them, the use of AMH seems to be widely accepted and has gained value in everyday clinical practice. AMH is a member of TGF-b glycoprotein superfamily, mainly expressed in granulosa cells of growing antral and pre-antral follicles in the gonadotropin independent phase [4]. AMH inhibits follicle sensitivity to follicle-stimulating hormone (FSH) and therefore affects follicular growth [5]. In clinical practice, AMH has been found to have high specificity and sensitivity in predicting ovarian response to Controlled Ovarian Stimulation (COS). Positive correlation with oocyte retrieval, role in poor responders’ prediction and a relation with life birth rate after IVF have also been noted [6–9]. AMH declines during reproductive age from puberty to menopause until it is almost undetectable [10, 11]. The idea of age related ovarian reserve diminishment and subsequent decline of ovarian function and reproductive potential have led scientist to seek for ovarian aging markers that could be used in practice as ovarian reserve markers.
Oxidative stress and ovarian aging
It is known that aerobic organisms develop the ability to use oxygen to efficiently emit energy. The prevention of oxidation during this procedure is controlled by antioxidant defense mechanisms and is of great importance. Any imbalance of the available antioxidant mechanisms combined with uncontrolled oxidation of biomolecules, mainly by the reactive oxygen species (ROS), results in oxidative stress. Many types of molecules like nucleic acids, proteins, lipids and carbohydrates may be damaged by oxidative stress suggesting that proteins, membranes and carbohydrate complexes could be victims of oxidative stress resulting in unrepaired DNA damage, telomerase loss, altered proteins and lipid destruction. These catastrophic oxidative events accumulate with age, cause tissue damage and in humans plays a significant role in the pathophysiology of many pathological situations and diseases, including the age related ovarian quality and quantity decline [12,13]. Thus, oxidative stress has been proposed to be involved in the pathogenesis of infertility. ROS concentrations have been proposed by many researchers to affect negatively fertilization and implantation [14]. More recently, the Advanced Glycation End products (AGEs) have been proposed to get involved in ovarian function decline [15, 16].
Advanced Glycation end products (AGEs), are the products of one of the most important modifications that occurs after translation, the nonenzymatic glycation of proteins, lipids, and nucleic acids [17, 18]. AGEs may either cause the formation of cross links between key molecules in the basement membrane of the extracellular matrix (ECM) or act via binding to receptors. Two types of receptors have been described. The first one is the multi-ligand transmembrane receptor, the RAGE (receptor for advanced glycation end products), known as the inflammatory receptor [17, 18]. RAGEs are expressed by several cell types, like endothelium, smooth muscle cells and ovaries and their activation may lead to unfavorable cellular conditions like proinflammation, cellular toxicity, and cellular damage via activating nuclear factor-κB [19, 20]. The second receptor that has been described is the soluble RAGE (sRAGE). sRAGE is an extracellular form of RAGE, lacking the cytosolic and transmembrane domains. It is able to adverse intracellular effects AGEs can cause and therefore is known as anti-inflammatory receptor [17, 18].
Prolonged exposure to AGEs, during reproductive life, has been shown to be able to cause subtle oxidative damage to the follicles of the ovary by altering ovarian microenvironment. These changes in the ovarian microenvironment may have adverse effects on granulosa cells’ metabolism, in antioxidant defense, and the development of inadequate follicle vascularization with subsequent follicle hypoxia. Follicle health and maturation may be negatively affected and age related oocyte dysfunction events may occur [21]. Additionally, it has been found that ff sRAGE levels were higher in younger women than in advanced aged women undergoing IVF treatment [22].The idea that sRAGEs may have a protective role in these unfavorable events have led scientist to investigate the correlation of sRAGEs with ovarian reserve markers.
Ovarian reserve markers in PCOS
AMH levels in women with PCOS have been shown to be two to three times higher than in healthy controls and levels of AMH are on average 75 times higher in granulosa cells from PCOS ovaries, compared to levels in granulosa cells from normal ovaries because of the increased development of antral follicles compared to normal women [23,24]. Serum AMH has been shown to be a diagnostic marker of high specificity (92%) and sensitivity (67%) for PCOS [24].
Serum AGE levels and AGE-RAGE expression in theca and granulosa cells have been found to be higher in PCOS women than in healthy controls. This has been attributed to hyperglycemia, oxidative stress and insulin resistance in PCOS women [25, 26] and is linked to diminished ovarian reserve and abnormal folliculogenesis [27]. On the contrary, follicular fluid sRAGEs have been found to be lower in women with PCOS compared to non-PCOS women [28, 29].
It has been shown, in vitro, that the inappropriate prolonged activation of ERK1/2 path, which is critical for normal follicle growth and the beginning of ovulation, by AGEs via intervention in the action of LH, could be responsible for the impaired follicle growth and the subsequent ovulation dysfunction that characterizes PCOS women. Moreover, it is understood that AGEs accumulation in FF of PCOS women could lead to premature ovarian aging [30].
Methods & Materials
49 women from different regions of Greece, mainly from Thrace, who received IVF treatment in the IVF Department of University Hospital of Alexandroupolis from December 2014 to May 2015 were recruited for this study and were divided in two groups (Group A and Group B) . Group A consisted of 38 non PCOS women, while Group B of 12 PCOS women diagnosed under the Rotterdam criteria. Written consent was signed by all women.
Controlled Ovarian Stimulation (COS) was offered to all women, after preliminary control and appropriate COS protocol was chosen for each after study and evaluation of parameters like age, day 3 serum FSH, day 3 serum LH, serum AMH and others. During COS period all women were offered serial ultrasound examinations and serum Estradiol (E2) measurements in order to evaluate respond to stimulation. I.M b-HCG administration was decided when at least 3 of developing follicles reached diameter of 18 mm and oocyte retrieval (OR) was planned for 36 hours post. During OR, FF needed to measure AMH and s RAGEs was collected.
Follicular Fluid collection
During oocyte retrieval, follicular fluid was aspired and collected in tubes. The embryologist separated the oocytes in FF and placed them in a plate with culture substances. Meanwhile, FF was collected in a falcon and labeled with woman’s name. Following FF was centrifuged for 15 minutes in 3000 rpm, to remove any unnecessary element, like cumulus cells. After centrifugation was completed, supernatant serum was transferred to another falcon (labeled with woman’s name) and refrigerated in -70 degree of Celsius. This procedure was followed in all cases in order to collect the samples.
Moreover, in order to be able to distinguish PCOS from non PCOS samples, falcons were labeled with respective labels. Therefore, the samples of Groups A and B could easily be evaluated and compared. AMH and sRAGE measurements were carried out simultaneously by the same kit, special for each parameter. AMH was measured by Elisa method, according to kit’s manufacturer (Anshlab) instructions (UltraSensitive AMH/MIS ELISA AL-105-i). The kit Quantikine ELISA/ Human RAGE was used for the measurements for the FF sRAGE levels according to manufacturer’s instructions(R & D Systems).
Statistical Analysis
The IBM SPSS Statistics for Windows Program, Version 21.0. Released 2012, Armonk, NY: IBM Corp. was used for the statistical analysis in our study.
Demographic characteristics and clinical data of women recruited were evaluated by descriptive statistic methods. The ratio of MII oocytes to the total number of oocytes retrieved for each woman was defined as simple quantitative expression of Oocyte quality. We consider that this ratio adequately represents oocyte quality and were used as quantitative variable during analysis. T-test for independent variables was used to compare the quantitative variables between two groups while χ2 test was used to compare the qualitative variables. Significance levels for both cases was set at 0, 05.
The concentrations of the parameters studied (serum and FF AMH, FF sRAGE) were calculated and presented as mean values ± standard deviation for each group separately. The comparison of these concentrations between the two groups was made by t-test for independent variables with significance level of 0.05.
In each group, quantitative variables were examined for possible monofactor linear correlation among them by the Pearson correlation coefficient r and the relative p-values. Multifactor linear regression was applied to whole sample, in order to study the correlation of ff sRAGE, ff AMH and serum AMH levels, taking into consideration women’s age, BMI and PCOS presence. The results of this multifactor analysis were expressed via βήτα coefficient (βήτα mean value± standard error) and the relative p-values. In the mono factor and in the multifactor analysis the significance level was of 0.05.
Results
In the beginning, we completed the above analysis between the two groups, including all qualitative and quantitative variables we had collected. The demographic and clinical characteristics of all women are presented in Table 1. Infertility in non PCOS women was attributed to tubal factor (21, 6%), to male factor (24, 3%), to premature ovarian failure (8, 1%), to other factors (8, 1%), to more than one factors (18, 9%) or was unknown (18, 9%). PCOS women presented in great percentage more than one infertility factors (50%). PCOS women had higher E2 levels when compared to non PCOS women, had more growing follicles during stimulation, more oocytes after OR. They also had more MII oocytes and more embryos available for embryo transfer (p-value <0, 05). There were no other statistical significant differences between the two groups in the clinical and laboratory characteristics studied.
Table 1. Demographic and clinical characteristics of 49 recruited women (12 PCOS and 37 non PCOS). Quantitative variables: mean value± standard deviation, comparison with t-test for independent samples. Quantitative variables: number of patients, percentage within parenthesis, comparison with χ2 test. NS: statistically non significant, significance level 0.05.
|
Characteristics |
PCOS women |
Non-PCOS women |
p- value |
|
Age |
34,0 ± 4,2 |
36,3 ± 5,5 |
NS |
|
ΒΜΙ |
22,8 ± 5,3 |
25,9 ± 4,7 |
NS |
|
Day 3 FSH (mIU/ml) |
6,8 ± 2,1 |
8,9 ± 3,6 |
NS |
|
Day 3 LH (mIU/ml) |
5,4± 2,1 |
5,27 ± 1,91 |
NS |
|
Smoking (cigarettes/day) |
5,0± 7,6 |
7,2 ± 8,8 |
NS |
|
Alcohol (glasses/week) |
0,41 ± 1,44 |
0,55 ± 1,96 |
NS |
|
Total Gonadotrophin administrated for COS (IU’s) |
2636 ± 2048 |
3600 ± 1191 |
NS |
|
E2 during COS |
3875 ± 2826 |
2200 ± 2197 |
0,04 |
|
Number of follicles |
9,8 ± 2,8 |
7,4 ± 3,7 |
0,04 |
|
Serum AMH (ng/ml) |
13,8 ± 22,7 |
4,6 ± 4,7 |
NS |
|
Follicular fluid AMH (ng/ml) |
3,1 ± 4,0 |
2,3 ± 2,1 |
NS |
|
Follicular fluid sRAGE (pg/ml) |
6237 ± 2784 |
4058 ± 1907 |
<0,01 |
|
Number of oocytes |
12,0 ± 5,9 |
5,2 ± 3,7 |
<0,01 |
|
Number of MII oocytes |
8,7 ± 5,2 |
3,5 ± 3,2 |
<0,01 |
|
Number of MII oocytes/ number of oocytes |
0,76 ± 0,22 |
0,62 ± 0,32 |
NS |
|
Number of embryos suitable for embryo transfer |
6,1 ± 3,7 |
2,5 ± 2,3 |
<0,01 |
|
Infertility Factor |
|
|
|
|
PCOS |
6 (50%) |
|
|
|
Tubal |
|
8 (21, 6%) |
|
|
Male |
|
9 (24, 3%) |
|
|
Premature ovarian insufficiency |
|
3 (8, 1%) |
|
|
Unknown |
|
7 (18, 9%) |
|
|
Other (Age, uterine abnormality, endometriosis) |
|
3 (8, 1%) |
|
|
Combined(more than one factor) |
6 (50%) |
7 (18, 9%) |
|
|
Pituitary Suppression |
|
|
NS |
|
GnRH agonist |
4 (33, 3%) |
12 (32, 4%) |
|
|
GnRH antagonist |
4 (33, 3%) |
19 (51, 4%) |
|
|
Cumulus-oocyte complex quality |
|
|
NS |
|
Normal |
9 (75%) |
25 (67, 6%) |
|
|
IMMCC, PMCC, POCC |
3 (25%) |
12 (32, 4%) |
|
|
Fertilization method |
|
|
NS |
|
IVF |
4 (33, 3%) |
6 (16, 2%) |
|
|
ICSI |
7 (58, 3%) |
26 (70, 3%) |
|
|
IVF- ICSI |
1 (8, 3%) |
3 (8, 1%) |
|
|
PREGNANCY |
|
|
NS |
|
βhCG (+) |
3 (25%) |
4 (10, 8%) |
|
|
Other IVF outcome |
9 (75%) |
33 (89, 2%) |
|
|
Total |
12 (100%) |
37 (100%) |
|
Following, we made the below analysis and the graphic with the data of serum AMH, FF AMH and FF sRAGEs.
Serum AMH, FF AMH and FF sRAGEs levels of PCOS and non PCOS women are presented in Table 2 and in Figure 1. PCOS women were found to have higher FF sRAGE levels compared to non PCOS women (p-value <0, 01). On the contrary, the differences in serum and FF AMH levels were not found to be statistically significant between the two groups. Moreover, the deviation of the values (standard deviation) of the three factors studied is larger in PCOS women. This could be attributed to the small sample size (12 women) or could reflect the real heterogeneity of PCOS women, indeed.
Table 2. Serum AMH, FF AMH and FF sRAGE studied in 12 PCOS and in 27 non PCOS women. Mean values ± standard deviations are presented, comparison with t-test for independent samples. NS: statically non significant with significance value 0.05.
|
Factor |
PCOS women |
non PCOS women |
p- value |
|
Serum AMH (ng/ml) |
13,8 ± 22,7 |
4,6 ± 4,7 |
NS |
|
Follicular Fluid AMH (ng/ml) |
3,1 ± 4,0 |
2,3 ± 2,1 |
NS |
|
Follicular Fluid sRAGE (ng/ml) |
6,2 ± 2,7 |
4,0 ± 1,9 |
<0,01 |
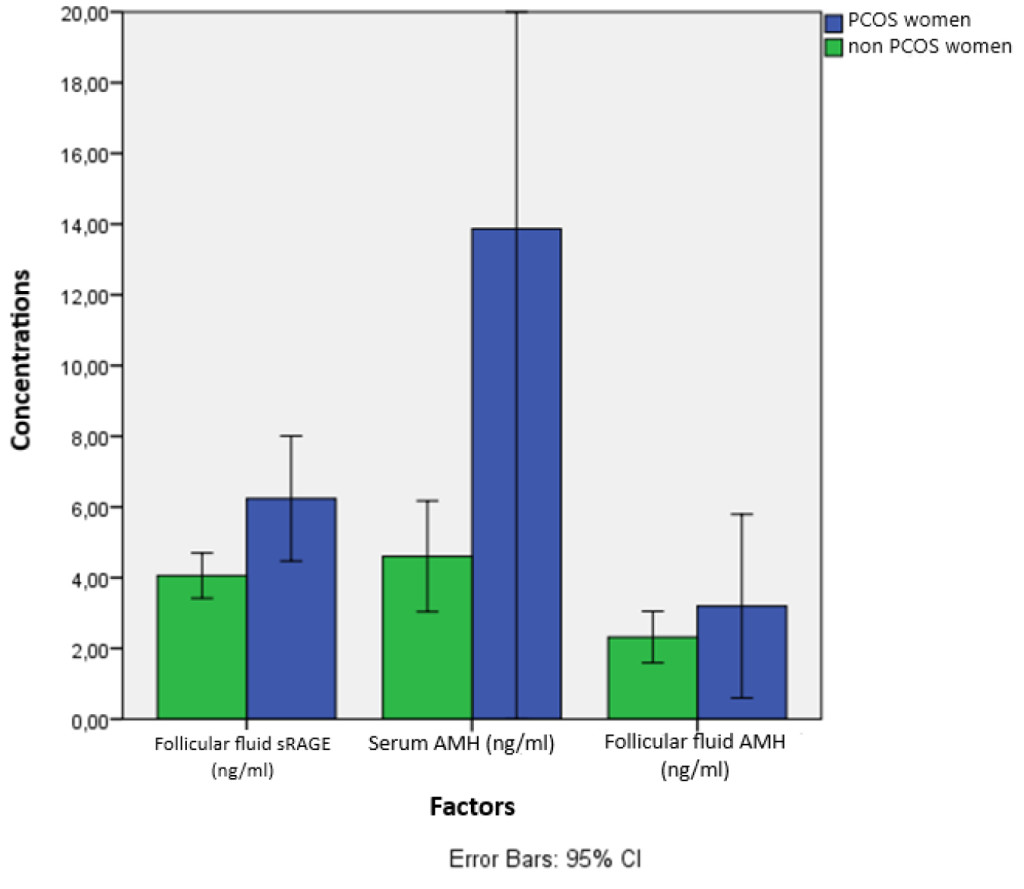
Figure 1. AMH and sRAGEs concentrations studies in serum and FF of 12 PCOS and 37 non PCOS. Mean values with 95% confidential intervals are presented.
This data is presented in the graph below (Figure 1).
Additionally, a multifactor analysis, regarding the three variables was made. The results were as following:
The most significant results of the monofactor analysis are presented summarized in Table 3. In PCOS women serum AMH, ff AMH and FF sRAGE levels were not found to be correlated with the number of the oocytes retrieved, the number of MII oocytes, with the embryo number or the ratio of MII oocytes to the total number of the oocytes retrieved. Serum AMH but not ff AMH was found to be a better marker of ovarian response in non PCOS women because it was found to be correlated with the number of MII oocytes and the number of the embryos available for embryo transfer. Only in non PCOS women, ff sRAGE levels were found to be negatively correlated with the quality of the oocytes, as it is expressed in the above mentioned ratio (r= -0.484, p-value= 0.003). This correlation is the most important finding of our study and is presented as a graph in Figure 2. Specifically, elevated ff sRAGE concentrations have been found to lead to lower Oocyte quality in non PCOS women. In PCOS women a high degree linear correlation of serum AMH and ff AMH, something that is not seen in non PCOS women, is noted (r= 0,965, p-value <0.001) (Figure 3). Neither serum AMH, nor ff AMH was found to be correlated with ff sRAGE levels in the sample studied. Lastly, ff sRAGE was found to have a negative correlation with BMI in non PCOS women (r= -0.401, p-value=0.014, Figure 4).
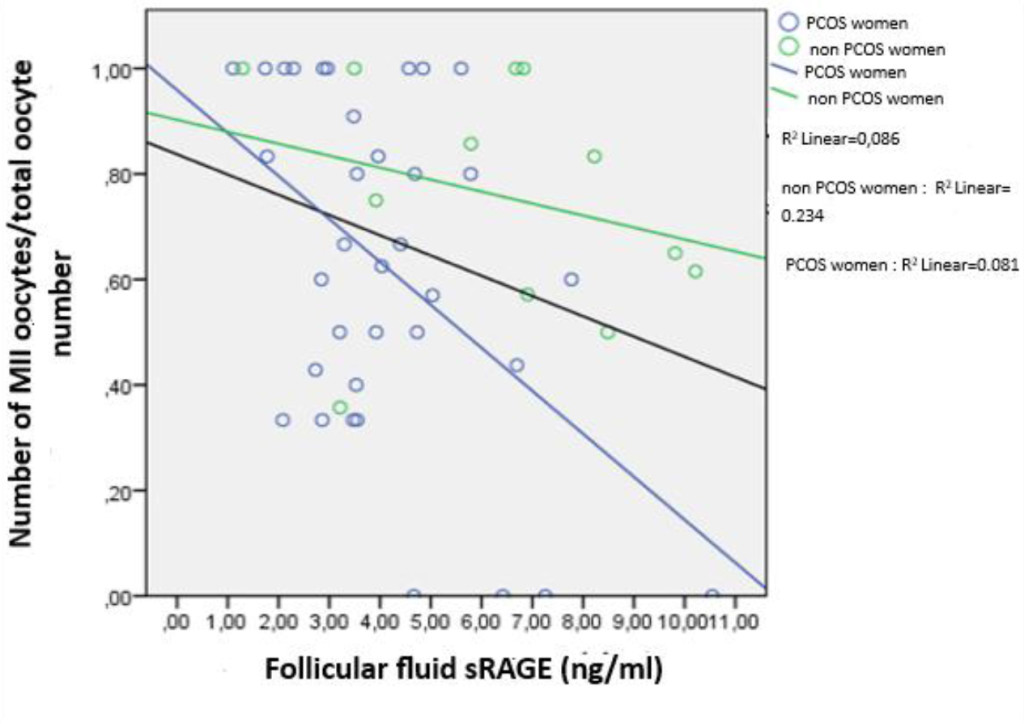
Figure 2. Graph of the correlation of number of MII oocytes/total Oocyte number with the concentration of ff sRAGE in 12 PCOS and 37 non PCOS women. Statistical significant correlation was noted only in non PCOS women (Pearson r = -0.484, p-value = 0.003).
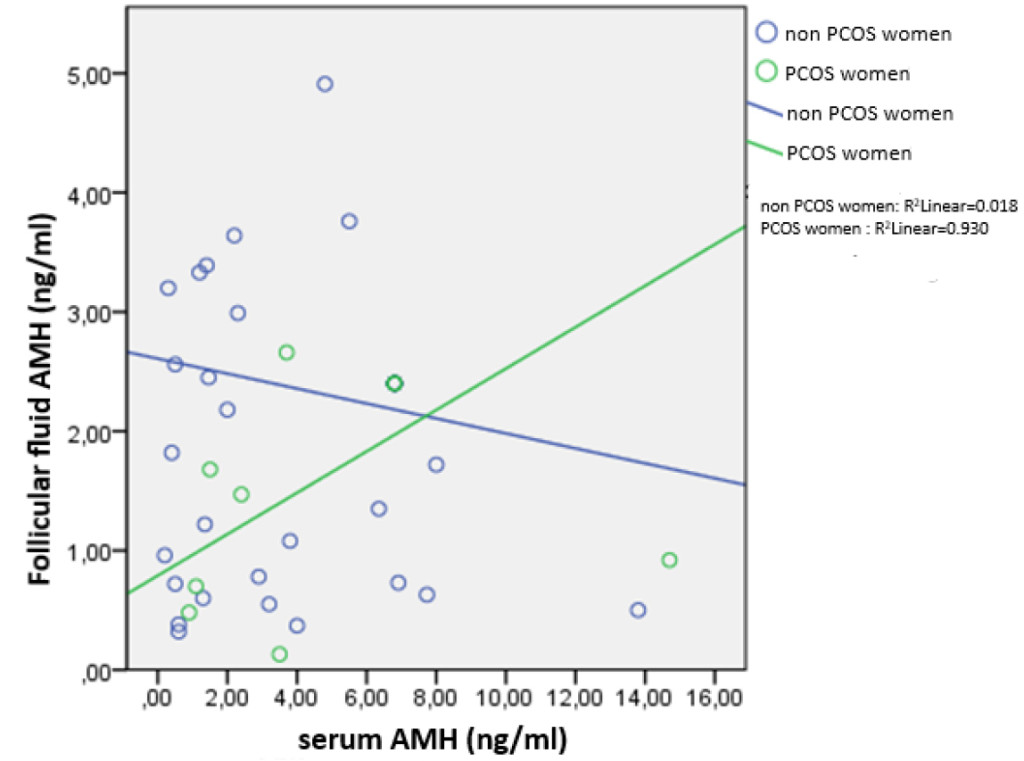
Figure 3. Graph of the correlation of serum AMH with ff AMH in 12 PCOS and in 37 non PCOS women. Statistical significant correlation only in PCOS women (Pearson r=0.965, p-value <0.001).
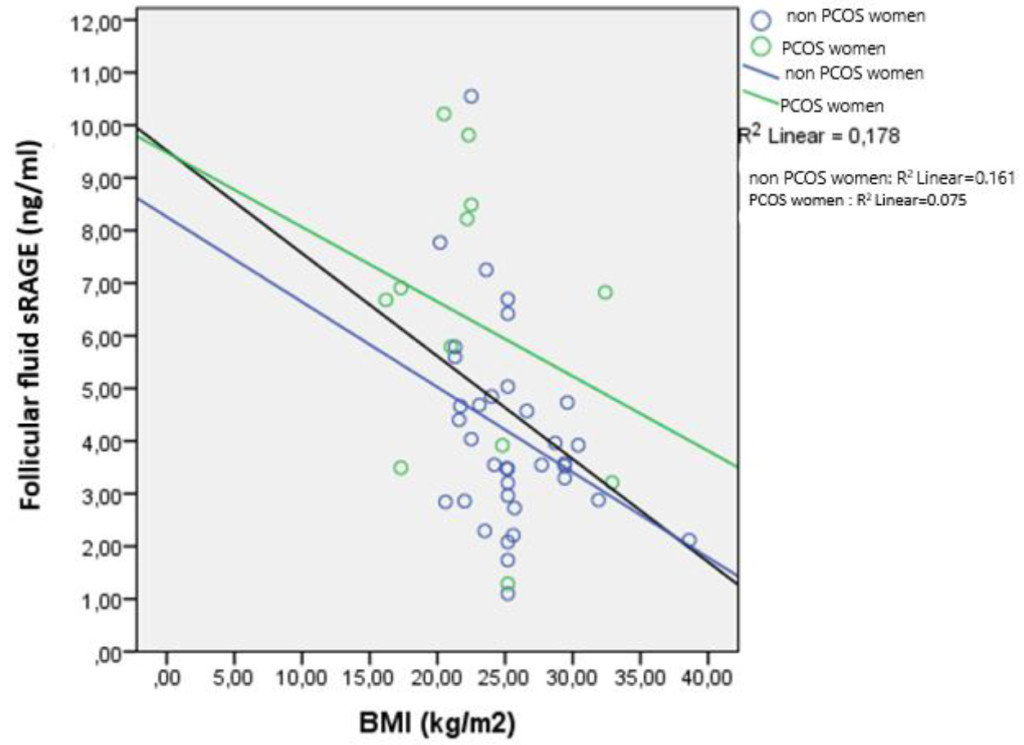
Figure 4. Graph of the correlation of ff sRAGE with the BMI of 12 PCOS and 37 non PCOS women. Statistically significant correlation is noted only in non PCOS women (Pearson r = -0.484, p-value = 0.003).
Table 3. Results of correlation of serum AMH and FF AMH with oxidative stress factors (ff SRAGEs) and with other clinical and laboratory factors in 12 PCOS and in 37 non PCOS women. Mono factor linear correlation based on Pearson’s r. NS: statistically non significant with significance levels 0.05%.
|
Factor correlation |
PCOS women |
Non PCOS women |
||
|
|
Pearson r |
p- value |
Pearson r |
p- value |
|
Number of oocytes , serum AMH |
|
NS |
0,287 |
NS (0,08) |
|
Number of oocytes, FF AMH |
|
NS |
|
NS |
|
Number of oocytes , FF sRAGE |
|
NS |
|
NS |
|
Number of MII oocytes, serum AMH |
|
NS |
0,413 |
0,011 |
|
Number of MII oocytes, FF AMH |
|
NS |
|
NS |
|
Number of MII oocytes, FF sRAGE |
|
NS |
|
NS |
|
Number of MII oocytes/ Number of oocytes, serum AMH |
|
NS |
|
NS |
|
Number of MII oocytes/ Number of oocytes, FF AMH |
|
NS |
|
NS |
|
Number of MII oocytes/ Number of oocytes, FF sRAGE |
|
NS |
-0,484 |
0,003 |
|
Number of embryos, serum AMH πλάσματος |
|
NS |
0,362 |
0,028 |
|
Number of embryos, FF AMH |
|
NS |
|
NS |
|
Number of embryos, FF sRAGE |
|
NS |
|
NS |
|
Serum AMH, FF AMH |
0,965 |
<0,001 |
|
NS |
|
Serum AMH, FF sRAGE |
|
NS |
|
NS |
|
FF AMH, FF sRAGE |
|
NS |
|
NS |
|
Seum AMH, IU’s gonadotrophins |
|
NS |
-0,387 |
0,018 |
|
FF AMH, IU’s gonadotrophins |
|
NS |
-0,387 |
0,022 |
|
FF sRAGE, ΒΜΙ |
|
NS |
-0,401 |
0,014 |
|
Number of oocytes, age |
|
NS |
-0,474 |
0,003 |
|
Number of oocytes, FSH |
|
NS |
-0,340 |
0,039 |
|
Number of oocytes, IU’s gonadotrophins |
-0,550 |
NS (0,06) |
-0,445 |
0,006 |
|
Number of oocytes, E2 |
0,577 |
0,049 |
0,293 |
NS (0,07) |
|
Number of oocytes, number of follicles |
0,610 |
0,035 |
0,545 |
<0,001 |
|
Number of MII ωαρίων, number of oocytes |
0,812 |
0,001 |
0,874 |
<0,001 |
|
Number of MII ωαρίων/number of oocytes, FSH |
|
NS |
-0,336 |
0,049 |
|
Number of embryos, FSH |
|
NS |
-0,385 |
0,018 |
|
Number of embryos, ΒΜΙ |
0,780 |
0,003 |
|
NS |
|
Number of embryos, IU’s gonadotrophins |
-0,579 |
0,049 |
-0,319 |
0,050 |
|
Number of embryos, number of oocytes |
0,720 |
0,008 |
0,777 |
<0,001 |
|
Number of embryos,number of MII oocytes |
0,758 |
0,004 |
0,917 |
<0,001 |
|
Number of embryos, Number of MII oocytes/ number of oocytes |
|
NS |
0,504 |
0,002 |
|
Number of follicles , age |
-0,840 |
0,001 |
-0,448 |
0,005 |
|
IU’s gonadotrophins, age |
|
NS |
0,526 |
0,001 |
|
IU’s gonadotrophins, FSH |
|
NS |
0,361 |
0,028 |
Lastly, with multifactor linear regression in all women, taking into consideration the age, serum AMH and ff AMH levels, we found that ff sRAGE levels is independently correlated only with the BMI (β= -136.1, p-value =0.036) and the presence of PCOS(β= 1563.9, p-value = 0,045).
Discussion
In our study we tried to determine whether FF sRAGEs are correlated to serum AMH or FF AMH levels and to evaluate the association of these markers with IVF outcome parameters, in PCOS women receiving IVF treatment.
AHM has been widely used as an ovarian reserve marker in prediction of IVF outcome [8]. Additionally, many researchers have found that the severity of PCOS is positively correlated with the number of small antral follicles and that AMH plays a significant role in the pathogenesis of anovulation in women with PCOS. However, in our study, AMH values between PCOS and non PCOS women were not found to be statistically significant. Additionally, we did not find a correlation between ff AMH and serum AMH. Regarding the predictive value of AMH in IVF outcome, serum AMH was found to be correlated with the number of the number of MII oocytes and the number of the embryos only in non PCOS women. We did not find a correlation of ff AMH with the number of the oocytes retrieved or the number of the embryos available for embryo transfer neither in PCOS, nor in non PCOS women.
As above mentioned, AGEs have been incriminated for age-related ovarian dysfunction due to the effect of oxidative stress mechanisms in the ovarian microenvironment that results in insufficient vascularization, hypoxia of the ovary and malnutrition of the granulosa cells [21]. It is known that folliculogenesis is an inflammatory procedure and when combined with COS during IVF cycles large amounts of cytokines are produced and secreted into the follicular fluid. This environment could cause a huge AGE production and effect negatively oocyte quality. Jinno et al, in a study of 157 women undergoing IVF treatment (71 PCOS women included) reported that elevated AGE levels play a significant role in ovarian dysfunction and are associated with poor IVF outcome [31]. While, AGEs have been found to have negative correlation with follicular growth and IVF outcome, in 2014 Merhi et al was the first to report that FF sRAGEs are positively correlated with ovarian reserve, as measured by FF AMH (r=0.5, P = 0.0085) and the number of the oocytes retrieved (r=0,57, P=0.02) but only in non-PCOS women [16]. Recently Li et al, who studied 124 women undergoing IVF treatment, divided into two age groups, found that ff sRAGE levels are positively correlated with folliculogenesis and IVF outcome only in women of advanced age [22].
In our study, we did not find a statistically significant correlation between ff sRAGE levels and the number of the oocytes retrieved or the number of the embryos available for embryo transfer after the IVF treatment in none of the groups studied. But we did found that ff sRAGE levels seem to have an effect on the quality of the oocytes retrieved. In fact, we found that increased ff sRAGE levels are negatively correlated with the quality of the oocytes retrieved, as defined by the ratio of MII oocytes to the total number of the oocytes retrieved but only in non PCOS women(r= -0.484, p-value= 0.003). Given that the number of the embryos available for embryo transfer is correlated with the number and the quality of the oocytes retrieved, it seems that ff sRAGEs play a role in the IVF outcome, at least in non PCOS women. On the contrary to this hypothesis, it has been shown by Malickova et al, that FF sRAGE concentrations in women undergoing IVF were significantly higher in those having a positive IVF outcome [31].
We also found that PCOS women have higher FF sRAGE levels when compared to non PCOS women (p-value <0,01)but no correlation of these high FF sRAGE values with IVF outcome parameters were noted in this group as above mentioned. On the contrary to our study, Wang et al found that FF sRAGEs are significantly decreased in PCOS females compared to control groups and associated with lower total gonadotrophin doses. However, they did also not found a correlation o FF sRAGEs with other IVF outcome parameters (number of oocytes retrieved, fertilization rate, number of high quality embryos) [28].
Lastly, we found a negative correlation of FF sRAGE levels with BMI(r= -0.401, p-value=0.014). No correlation with FF sRAGE and women’s age was noted.
Therefore combining the above mentioned information and taking into consideration the small sample size, we can conclude that there is no correlation between the AMH protein and the oxidative stress agents. However, each of these factors could be used separately for the improvement and the prediction of IVF outcome. AMH can be used as an ovarian reserve marker and as a predictive marker of ovarian response during ovarian stimulation. On the other hand, FF oxidative stress agents (sRAGEs) could consist of a great marker of the quality of the oocytes retrieved during IVF treatment and an indirect marker of IVF outcome. The combination of both could be used, therefore, in order to improve the IVF outcome.
References
- Stein I, Leventhal M (1935) Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 29: 181–5
- Yildiz BO, Bozdag G, Yapici Z, Esinler I, et al. (2012) Prevalence, phenotype and cardiomatabolic risk of polycystic ovary syndrome under different diagnostic criteria. Hum. Reprod 27: 3067–73.
- Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB (2006) A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update 12: 685–718. [crossref]
- Dewailly D, Andersen CY, Balen A, Broekmans F, Dilaver N, et al. (2014) The physiology and clinical utility of anti-Mullerian hormone in women. Hum Reprod Update 20: 370–385. [crossref]
- Pellatt L, Rice S, Dilaver N, et al. (2011) Anti-Müllerian hormone reduces follicle sensitivity to follicle-stimulating hormone in human granulosa cells. Fertil Steril 96: 1246–12451.e,
- RiggsRM, DuranEH, BakerMW, KimbleTD, et al. (2008) Assessment of ovarian reserve with anti-Müllerian hormone: a comparison of the predictive value of anti-Müllerian hormone, follicle-stimulating hormone, inhibin B, and age. Am J Obstet Gynecol 199: 202.e1–8.
- Broer SL, van Disseldorp J, Broeze KA, et al. (2013) IMPORT study group. Added value of ovarian reserve testing on patient characteristics in the prediction of ovarian response and ongoing pregnancy: an individual patient data approach. Hum Reprod Update 19: 26–36,
- La Marca A, Sighinolfi G, Radi D, Argento C et al. (2010) Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update 16: 113–30.
- Nelson SM, Yates RW, Fleming R (2007) Serum anti-Müllerian hormone and FSH: prediction of live birth and extremes of response in stimulated cycles–implications for individualization of therapy. Hum Reprod 22: 2414–2421. [crossref]
- La Marca A, Orvieto R, Giulini S, Jasonni VM et al. (2004) Mullerian-inhibiting substance in women with polycystic ovary syndrome: relationship with hormonal and metabolic characteristics. Fertil Steril 82: 970–972.
- Laven JS, Mulders AG, Visser JA, Themmen AP et al. (2004) Anti-Mullerian hormone serum concentrations in normoovulatory and anovulatory women of reproductive age. J Clin Endocrinol Metab 89: 318–323
- Betteridge DJ (2000) What is oxidative stress? Metabolism 49: 3–8. [crossref]
- Kirkwood TB (2008) Understanding ageing from an evolutionary perspective. J Intern Med 263: 117–127. [crossref]
- Ashok Agarwal, Sajal Gupta, Rakesh K. Sharma (2005) Role of oxidative stress in female reproduction, Reprod Biol Endocrinol 3: 28
- Stensen MH, Tanbo T, Storeng R, Fedorcsak P (2014) Advanced glycation end products and their receptor contribute to ovarian ageing. Hum Reprod 29: 125–134. [crossref]
- Merhi Z, Irani M, Doswell AD, Ambroggio J. Follicular fluid soluble receptor for advanced glycation end-products (sRAGE): a potential indicator of ovarian reserve. J Clin Endocrinol Metab 99: E226–33.
- Inagi R (2011) Inhibitors of advanced glycation and endoplasmic reticulum stress. Methods Enzymol 491: 361–380. [crossref]
- Piperi Ch, Adamopoulos Ch, Dalagiorgou E, Diamanti-Kandarakis E et al. (2012) Crosstalk between Advanced Glycation and Endoplasmic Reticulum Stress: Emerging Therapeutic Targeting for Metabolic Diseases. The Journal of Clinical Endocrinology & Metabolism 97: 2231–2242.
- Schmidt AM, Yan SD, Yan SF, Stern DM (2000) The biology of the receptor for advanced glycation end products and its ligands. Biochim Biophys Acta 1498: 99–111. [crossref]
- Fujii EY, Nakayama M (2010) The measurements of RAGE, VEGF, and AGEs in the plasma and follicular fluid of reproductive women: the influence of aging. Fertil Steril 94: 694–700. [crossref]
- Tatone C, Amicarelli F, Carbone MC, Monteleone P, Caserta D, et al. (2008) Cellular and molecular aspects of ovarian follicle ageing. Hum Reprod Update 14: 131–142. [crossref]
- Li YJ, Chen JH, Sun P, Li JJ1 et al. Intrafollicular soluble RAGE benefits embryo development and predicts clinical pregnancy in infertile patients of advanced maternal age undergoing in vitro fertilization. J Huazhong Univ Sci Technolog Med Sci. 2017 Apr;37(2): 243–247. doi: 10.1007/s11596–017–1722-z. Epub 2017 Apr 11.
- Pellatt L, Hanna L, Brincat M, Galea R, Brain H, et al. (2007) Granulosa cell production of anti-Müllerian hormone is increased in polycystic ovaries. J Clin Endocrinol Metab 92: 240–245. [crossref]
- Pigny P, Jonard S, Robert Y, Dewailly D. Serum anti-Mullerian hormone as a surrogate for antral follicle count for definition of the polycystic ovary syndrome. J Clin Endocrinol Metab 91: 941–5.
- Pertynska-Marczewska M, Diamanti-Kandarakis E, Zhang J, Merhi Z (2015) Advanced glycation end products: a link between metabolic and endothelial dysfunction in polycystic ovary syndrome? Metab Clin Exp 64: 1564–73.
- Hu H, Jiang H, Ren H, Hu X, et al. (2015) AGEs and chronic subclinical inflammation in diabetes: disorders of immune system. Diabetes Metab Res Rev 31: 127–37.
- Merhi Z (2014) Advanced glycation end products and their relevance in female reproduction. Hum Reprod 29: 135–145. [crossref]
- Wang B, Li J, Yang Q, Zhang F, et al. (2017) Decreased levels of sRAGE in follicular fluid from patients with PCOS. Reproduction 153: 285–292. [crossref]
- Garg D, Grazi R, Lambert-Messerlian GM, Merhi Z (2017) Correlation between follicular fluid levels of sRAGE and vitamin D in women with PCOS. J Assist Reprod Genet.
- Diamanti-Kandarakis E, Piperi C, Livadas S, Kandaraki E, et al. (2013) Interference of AGE-RAGE Signaling with Steroidogenic Enzyme Action in Human Ovarian Cells. San Francisco, CA: Endocrine Society.
- Jinno M, Takeuchi M, Watanabe A, Teruya K et al. (2011) Advanced glycation end-products accumulation compromises embryonic development and achievement of pregnancy by assisted reproductive technology. Hum Reprod 26: 604–10.
- Malickova K, Jarosova R., Rezabek K, Fait T, et al. (2010) Concentrations of sRAGE in serum and follicular fluid in assisted reproductive cycles – a preliminary study. Clin Lab 56: 377–38