Abstract
Introduction: Aim of the study was to examine the occurrence of kissing molars from the nationwide Health 2000 Survey carried out on the Finnish adult population aged 30 years and older. Kissing molars refer to impaction of a mandibular third molar and a neighboring molar with occlusal surfaces facing towards each other. At present, prevalence of kissing molars at a national level is unknown.
Methods and materials: From the two-staged stratified cluster-sample of 8028 subjects, panoramic radiographs and clinical oral examinations were carried out for 5989 subjects (46% men, 54% women; mean age 52.5 years; SD 14.6; range 30?97). Radiographs were examined for presence of third molars and kissing molars. Clinical measurements included total number of clinically visible teeth and total number of molars. From the demographic data, age, gender, place of residence, and level of education were included. Statistical significances were evaluated with Fisher’s exact test and Mann-Whitney U test. SAS Callable SUDAAN software was used to obtain weighted distributions of kissing molars representative of the population aged 30 years and older, and separately of people with third molars.
Results: Kissing molars occurred in 0.05% of the adult population (5 per 10000 adult inhabitants) and in 0.1% of those subjects with third molars (10 per 10000 such subjects). In subjects with kissing molars, the mean numbers of clinically visible teeth (p = 0.021) and molars (p = 0.016) were smaller compared to those without kissing molars. The demographic features analyzed, showed no statistically significant association with the occurrence of kissing molars.
Conclusion: This is the first study published to date on the prevalence of kissing molars at the population level. The prevalence of kissing molars in the population was very small. For the sake of comparison, kissing molars are not seen as often as supernumerary teeth in third molar region.
Keywords
Adult, Health Survey, Molar, Third, Prevalence, Radiography, Panoramic, Tooth, Impacted
Introduction
Third molars are associated with common diseases, such as pericoronitis, but also with uncommon diagnoses, such as mandibular fractures, supernumerary teeth, and kissing molars. The prevalence of fractures related to extractions is between 0.0034% and 0.0075% [1]. Supernumerary teeth (i.e. fourth molars) occur with an incidence between 0.9% and 2.2% [2]. However, the prevalence of kissing molars at a national level is unknown, because population-based oral health studies do not usually include panoramic radiographs.
Kissing molars occur when a third molar is impacted together with the neighboring tooth, with occlusal surfaces facing towards each other. A Dutch researcher first described this phenomenon as “kissing molars” in a case report in the 1970s [3]. At present, most information about kissing molars derives from case reports. The third molar may be impacted together with the second molar [4–11] or with the fourth molar [11, 12–14]. Kissing molars may be an incidental finding from the panoramic radiograph [4, 8, 9, 15] or they may cause symptoms, such as pain, swelling, and suppuration [6, 7, 10, 11, 13, 14]. The age of the patient at diagnosis varies between 18 and 48 years [7, 15]. Treatment options consist of operative extraction, sometimes with sagittal split osteotomy, [9] or orthodontic treatment [16].
The aim of the study was to examine the occurrence of kissing molars at a national level from the population-based Health 2000 Survey with subjects aged 30 to 100 years. The nationwide material included both clinical oral examinations and panoramic radiographs.
Methods and Materials
Our study was part of the Health 2000 Survey [17] organized by the National Institute for Health and Welfare during the years 2000 and 2001 (BRIF8901, Bioresource Research Impact Factor). A sample of 8028 subjects was created with a two-staged, stratified cluster-sampling method representing the entire population aged 30 years or older [18]. The subjects reflected a population of 2806169 inhabitants aged 30 years or older [18]. The Health 2000 Survey included general health examination, interview, questionnaires, clinical oral examination, and a panoramic radiograph. After clinical oral examinations, 6115 panoramic radiographs were taken. Due to inaccuracy around the third molar area, 110 radiographs were excluded. After excluding 16 subjects that had participated only in the radiograph, the final sample consisted of 5989 subjects, of whom both clinical and radiographic data were enrolled. From the demographic data, age and gender were included as well as level of education (basic, medium, and high), and place of residence (city, town, and countryside). From the clinical data, total number of clinically visible teeth in the mouth and total number of molars were used. Among the subjects with kissing molars, clinical probing depth of the first molar adjacent to kissing molars and over-eruption of corresponding maxillary molars were observed.
Digital panoramic radiographs were taken with Planmeca 2002 CC Proline (Planmeca, Helsinki, Finland) equipment using 58 to 68 kV and 4 to 10 mA depending on the size of the subject. The first author examined the radiographs in relation to third molar findings using the Romexis software version 3.6.0.R (Planmeca, Helsinki, Finland). A subject with third molars was recorded if at least one third molar or a remnant of it was found in the panoramic radiograph. Kissing molars were defined as a finding with an impacted mandibular third molar and a neighboring molar – either a second molar or a supernumerary molar – with occlusal surfaces facing towards each other. If the occlusal surfaces were in inclined position towards each other, such teeth were named as “pseudo-kissing molars”. Identification of kissing molars was simple, but for accuracy of recognition of third molars, 47% of the radiographs were examined twice. The intra-examiner reliability of the measurements was defined from the 10% of radiographs that were re-examined: the agreement was 93% for recognition of third molars and the kappa-value was 0.882.
Occurrence of kissing molars was reported separately for all subjects and for those subjects with third molars. Analyses were computed with IBM SPSS Statistics software version 24 (IBM Corp., Armonk, NY, USA). Differences between subgroups were evaluated with Fisher’s exact test for frequencies and Mann-Whitney U nonparametric test for means of independent samples. SAS Callable SUDAAN software version 11.0.1 (Research Triangle Institute, Research Triangle Park, NC, USA) was used to account for the complex sampling method, and to obtain weighted distributions of kissing molars representative of whole population aged 30 years and older, and separately representative of all people with third molars.
Permission for the study was acquired from the National Institute for Health and Welfare. The subjects had signed a written informed consent before health examinations. Ethical approvals for the clinical and radiographic examinations were obtained from the Ethics Committee of the National Public Health Institute and the Ethics Committee of Epidemiology and National Health in the Hospital District. The protocol was in compliance with the 1964 Helsinki Declaration. A safety license was granted by the Radiation and Nuclear Safety Authority.
Results
Among our 5989 subjects, 46% were men and 54% were women, and the overall mean age was 52.5 years (SD 14.6; median 51; range 30–97 years). Altogether 2805 (47%) subjects had at least one third molar or a remnant of it; 54% were men and 46% women, and their mean age was 47.6 years (SD 12.2; median 46; range 30–93 years). The panoramic radiographs revealed three subjects with kissing molars, two men and one woman (Figure 1).
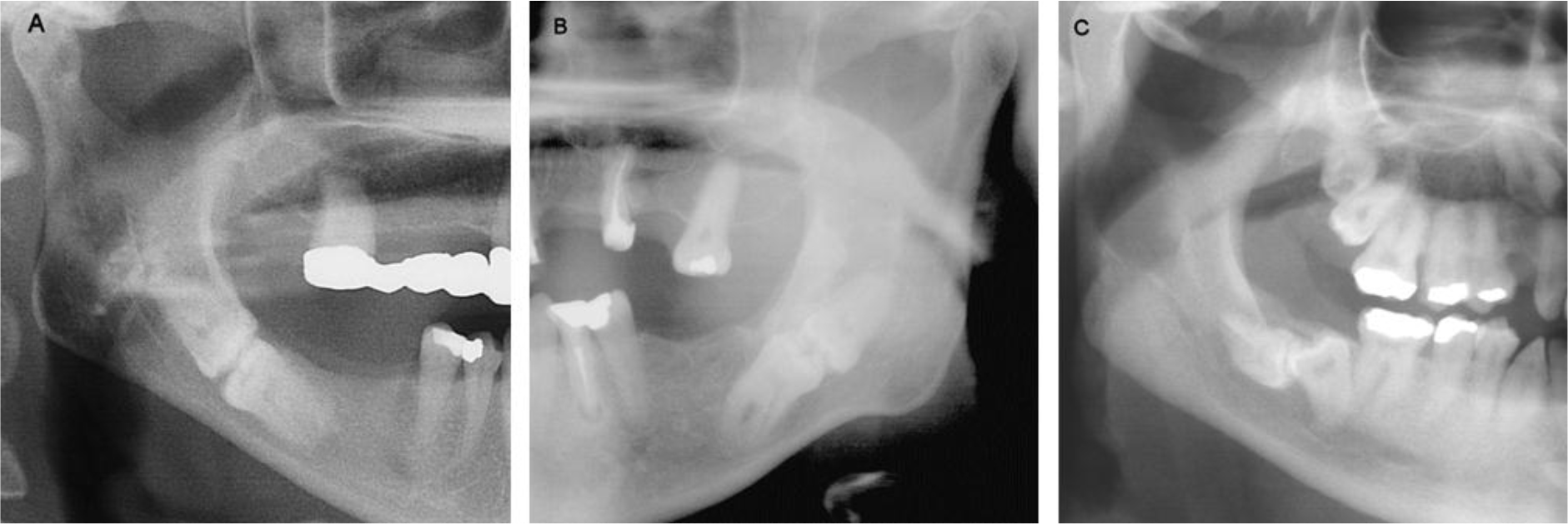
Figure 1. Cropped panoramic radiographs of the subjects with kissing molars. A. Impacted second and third molars on the right side in a 48-year-old woman. B. Impacted second and third molars on the left side in a 46-year-old man. C. Impacted second and third molars (pseudo-kissing) on the right mandible in a 39-year-old man with also other impacted teeth in the jaws.
Probing depth of the first mandibular molar adjacent to kissing molars in case C was clinically measured as 4?6 mm. Over-erupted maxillary molars opposite to kissing molars were not identified. In the analysis of the characteristics of all 5989 subjects with and without kissing molars, the demographic features showed no statistically significant association with the occurrence of kissing molars
(Table 1). In the subgroup of the 2805 subjects with third molars, there were two statistically significant differences between the groups: the mean number of clinically visible teeth (Mann-Whitney U statistic 7427.5, p = 0.021) and also the mean number of molars (Mann-Whitney U statistic 7565.0, p = 0.016) were smaller in subjects with kissing molars than in those without kissing molars (Table 2). The weighted distributions were as follows: kissing molars occurred in 0.05% (standard error SE 0.03) of the adult population and in 0.1% (SE 0.06) of those subjects with third molars. In other words, 5 per 10000 inhabitants and 10 per 10000 subjects with third molars had kissing molars.
Table 1. Comparison of characteristics of subject with kissing molars and without kissing molars in all 5989 subjects. The number of teeth refers to the total number of clinically visible teeth. The number of molars refers to the total number of clinically observed molars.
|
Characteristics |
With kissing molars (n = 3) |
Without kissing molars (n = 5986) |
P-value |
|
Age |
|
|
|
|
Mean (SD) years |
44.3 (4.7) |
52.5 (14.6) |
0.330a |
|
No. of teeth |
|
|
|
|
Mean (SD) |
19.0 (1.7) |
19.8 (10.7) |
0.315a |
|
No. of molars |
|
|
|
|
Mean (SD) |
3.0 (1.0) |
5.3 (3.8) |
0.299a |
|
Gender |
|
|
|
|
Male |
2 |
2747 (46%) |
0.597b |
|
Female |
1 |
3239 (54%) |
|
|
Educationc |
|
|
|
|
Basic |
2 |
2332 (39%) |
0.783b |
|
Medium |
1 |
1924 (32%) |
|
|
High |
0 |
1708 (29%) |
|
|
Place of residence |
|
|
|
|
City |
2 |
3648 (61%) |
0.498b |
|
Town |
1 |
858 (14%) |
|
|
Countryside |
0 |
1480 (25%) |
|
|
aMann-Whitney U non-parametric test. bFisher’s exact test. cLevel of education was not available for 22 subjects. |
|||
Table 2. Comparison of characteristics between subject with kissing molars and without kissing molars (n = 2805 subjects with third molars). The number of teeth denotes to total number of clinically visible teeth per subject. The number of molars denotes to total number of clinically detected molars per subject.
|
Characteristics |
With kissing molars (n = 3) |
Without kissing molars (n = 2802) |
P-value |
|
Age |
|
|
|
|
Mean (SD) years |
44.3 (4.7) |
47.6 (12.2) |
0.738a |
|
No. of teeth |
|
|
|
|
Mean (SD) |
19.0 (1.7) |
25.4 (6.2) |
0.021a |
|
No. of molars |
|
|
|
|
Mean (SD) |
3.0 (1.0) |
7.5 (2.9) |
0.016a |
|
Gender |
|
|
|
|
Male |
2 |
1519 (54%) |
0.563b |
|
Female |
1 |
1283 (46%) |
|
|
aMann-Whitney U nonparametric test. bFisher’s exact test. |
|||
Discussion
This is the first study published to date on the prevalence of kissing molars at the population level. The occurrence of kissing molars at 0.05% in our population was small. If it is compared to the prevalence of supernumerary teeth in the third molar region, it is found that supernumerary teeth (at 0.9% and 2.2%) are more common than kissing molars [2]. When the occurrence of kissing molars is compared to the incidence of mandibular fractures in relation to third molars, it is found that kissing molars are more common than fractures at 0.0034% and 0.0075% [1]. The occurrence of kissing molars at 0.05% in our population was about the same as the prevalence of 0.06% among all surgical patients at a university clinic [19]. Our occurrence at 0.1% in subjects with third molars was, however, only one-third of the 0.3% reported among third molar patients at a military hospital [20]. This discrepancy is explained by the fact that our sample represented the population, whilst the military-hospital study analyzed patient material.
In the first published case report, the kissing molars were second and third molars on both sides of the mandible [3]. Later, the terminology of kissing molars has been attributed also to other teeth, e.g. first and second molars [16, 20]. In the first case report, the occlusal surfaces were facing completely towards each other [3]. In recent case reports, teeth in inclined positions towards each other are also named as kissing molars [11, 15, 16, 19]. Such molars might be called “pseudo-kissing”. Therefore, we included in our analysis a case with pseudo-kissing molars in angulated (50 degrees) position towards each other (Figure 1C). The majority of the kissing-molar case reports were published in the 2000s, however, they failed to present the year of diagnosis of the patient. Therefore, it is difficult to decide whether the prevalence of kissing molars has increased during the 2000s, as the number of publications indicates. This increase of cases may be due to increased possibilities of imaging, but may also depend on an increased number of journals accepting case reports for publication. Similar examples of exceptional impaction of mandibular molars together with a neighboring tooth are already presented in older text books, for example in Stafne’s Oral Roentgenographic Diagnosis, at least from the third edition (1969) onwards [21]. Thus, kissing molars are not a new discovery, but the illustrative name was not used until 1973.
In our study, kissing molars showed no other pathology in the radiographs than impaction. However, pathological probing depth of the first molar in the case C was reported as 4–6 mm. Over-eruption of the maxillary molars was not observed in spite of long-standing absence of mandibular molars. Earlier studies have shown cases with enlarged follicular space, with a cyst, or resorption of the crown [6, 10, 11, 13, 14]. The majority of the earlier cases with pathology were younger than our subjects. For our cases, surveillance rather than surgery would be the preferred treatment of choice. However, the subjects should be informed about the presence of kissing molars.
Generally, younger age, female gender, and higher education are associated with good oral health [22]. It is not expected that demographic characteristics have an association with the development of kissing molars, but they may have a role in the behavior of the subject in seeking dental care. As regards kissing molars, the demographic features analyzed, i.e. age, gender, the level of education, and the place of residence, showed no statistically significant association with the occurrence of kissing molars, obviously due to the rarity of the phenomenon. However, our results showed that the total number of clinically visible teeth and also molars were smaller in subjects with kissing molars compared to those without such teeth. This may be explained by the chain reaction of long-standing absence of mandibular molars, followed by extraction of over-erupted maxillary molars, poor occlusion, and still more extractions.
In the literature, the age of diagnosis falls between 18 and 48 years, [7, 15] and 53% of subjects were younger than 30 years and 47% were 30 years or older. In our material, we had the age limit, and therefore, the youngest examined subjects were 30 years old. If the prevalence in the case reports and our material were similar, it might be extrapolated that in our material three subjects more could be found among subjects younger than 30 years. However, earlier extractions of third molars, perhaps also kissing molars, were not available in our data. By making deductions based on our results and earlier case reports, it can be estimated that almost 3000 adults in our country (with a population of 5.5 million) may have kissing molars. The presence of kissing molars imposes clinical implications on the subject. That is to say that kissing molars may weaken the mandibular bone. In traffic accidents, sports injuries, fighting, and falling, the fracture line likely goes through the impacted teeth in the angle of the mandible. This risk of fracture may also be evident in relation to extraction of these teeth. Due to the rarity of the phenomenon, scientific evidence on this is not available. It is concluded that in this first study published to date on the prevalence of this phenomenon at the population level, the prevalence of kissing molars in the population was very small. For the sake of comparison, supernumerary teeth in third molar region are slightly more common than kissing molars.
Acknowledgment: The field surveys were organized by the National Institute for Health and Welfare in Finland and partly funded by the Finnish Dental Society Apollonia, the Finnish Dental Association, and Planmeca Oy.
Conflict of interest:The authors declare that they have no competing interests.
References
- Joshi A, Goel M, Thorat A (2016) Identifying the risk factors causing iatrogenic mandibular fractures associated with exodontia. A systemic meta-analysis of 200 cases from 1953 to 2015. Oral Maxillofac Surg 20: 391–396. [crossref]
- Shahzad KM, Roth LE (2012) Prevalence and management of fourth molars: a retrospective study and literature review. J Oral Maxillofac Surg 70: 272–275. [crossref]
- Van Hoof RF (1973) Four kissing molars. Oral Surg Oral Med Oral Pathol 35: 284. [crossref]
- Robinson JA, Gaffney W Jr, Soni NN (1991) Bilateral ‘kissing’ molars. Oral Surg Oral Med Oral Pathol 72: 760. [crossref]
- McIntyre G (1997) Kissing molars: an unexpected finding. Dent Update 24: 373–374. [crossref]
- Krishnan B (2008) Kissing molars. Br Dent J 204: 281–282. [crossref]
- Scheuber S, Bornstein M (2014) Kissing molars. Ein spezieller radiologischer Befund. (German). Swiss Dent J 124: 16–17.
- Narayanankutty A, Velayudhannair V, Sunila T, Vineet AD, Thomas J, et al. (2015) Till surgery do us part: unexpected bilateral kissing molars. Clinics and Practice 5: 688–689. [crossref]
- Cansiz E, Isler SC, Gultekin BA (2016) Removal of deeply impacted mandibular molars by sagittal split osteotomy. Case Rep Dent Available: https://www.hindawi.com/journals/crid/2016/1902089/.
- Zerener T, Bayar GR, Altug HA, Kiran S (2016) Extremely rare form of impaction bilateral kissing molars: Report of a case and review of the literature. Case Rep Dent Available:https://www.hindawi.com/journals/crid/2016/2560792/.
- Arjona-Amo M, Torres-Carranza E, Batista-Cruzado A, Serrera-Figallo MA, Crespo-Torres S, et al. (2016) Kissing molars extraction: Case series and review of the literature. J Clin Exp Dent 8: 97–101. [crossref]
- Nakamura T, Miwa K, Kanda S, Nonaka K, Higash S, et al. (1992) Rosette formation of impacted molar teeth in mucopolysaccharidoses and related disorders. Dentomaxillofac Radiol 21: 45–49. [crossref]
- Bakaeen G, Baqain ZH (2005) Interesting case: kissing molars. Br J Oral Maxillofac Surg 43: 534. [crossref]
- Boffano P, Gallesio C (2009) Kissing molars. J Craniofac Surg 20: 1269–1270. [crossref]
- Kiran HY, Bharani S, Kamath RA, Manimangalath G, Madhushankar GS et al. (2014) Kissing molars and hyperplastic dental follicles: Report of a case and literature review. Chin J Dent Res 17: 57–63. [crossref]
- Barros SE, Janson G, Chiqueto K, Ferreira E, Rösing C (2018) Expanding torque possibilities: A skeletally anchored torqued cantilever for uprighting “kissing molars”. Am J Orthod Dentofacial Orthop 153: 588–598. [crossref]
- National Institute for Health and Welfare. Health 2000 in brief. Available: https://thl.fi/en/web/thlfi-en/research-and-expertwork/projects-and-programmes/health-2000–2011/health-2000-in-brief..
- Heistaro S (2008) Methodology report. Health 2000 Survey. Publications of the National Public Health Institute; B 26/2008. Helsinki; National Public Health Institute, Available: http://www.julkari.fi/bitstream/handle/10024/78185/2008b26.pdf?sequence =1.w
- Yanik S, Ayranci F, Isman Ö, Büyükçikrikci S, Aras MH (2017) Study of kissing molars in Turkish population sample. Niger J Clin Pract 20: 659–664. [crossref]
- Gulses A, Varol A, Sencimen M, Dumlu A (2012) A study of impacted love: kissing molars. Oral Health Dent Manag 11: 185–188. [crossref]
- Stafne EC (1969) Malposition of teeth. In: Stafne EC (ed). Oral Roentgenographic Diagnosis. Philadelphia, PA: WB Saunders Pg No: 42–54.
- Suominen-Taipale L, Nordblad A, Vehkalahti M, Aromaa A (eds). (2008) Oral health in the Finnish adult population. Health 2000 Survey. Publications of the National Public Health Institute B25/2008, Helsinki; National Public Health Institute, Available: http://www.julkari.fi/handle/10024/103030.