DOI: 10.31038/IRCI.1000102
Summary
Trigeminal nerve is a mixed nerve with a contingent of sensory fibers for integuments of the face, a contingent of driving fibers for the masticatory muscles and a contingent of autonomic fibers. Its nuclei are disseminated on the brainstem and it emerges from the middle of the pons, at the lateral surface of the brainstem by 2 driving and sensory roots that merge to the trigeminal ganglion.
We report an unilateral duplicity of the trigeminal nerve causing a sensorineural hearing loss caused by the conflict of the aberrant root and the vestibulocochlear nerve.
Keywords
Aberrant Emergency Nerve, MRI, Sensorineural Hearing Loss, Trigeminal nerve.
Introduction
The trigeminal nerve is the largest cranial nerve. It is a mixed nerve with a contingent of sensory fibers for integuments of the face, a contingent of driving fibers for the muscles of mastication and a contingent of autonomic fibers. Its nuclei are disseminated on the brainstem and it emerges from the middle of the pons, at the lateral surface of the brainstem by 2 driving and sensory roots that coalesce to form the trigeminal ganglion at the Meckel’s cave. Even if the variations of the path brain vessels are usual, the abnormalities of cranial nerves emergence are rare (Hypoglossal Nerve).
We report an unusual case of cisternal portion of trigeminal nerve duplicity, with aberrant emergency of one bundle responsible of a conflict with vestibulocochlear nerve.
Observation
Mr SD, 35, consulted for a unilateral left hearing loss since childhood without recent worsening. He does not feel tinnitus nor dizziness. The otoscopy is normal. The acoumetry is a unilateral left perception of hearing loss. The right ear is normal. Audiometric testing shows a sensorineural hearing loss of on average 60dB. The precocious Brainstem Auditory Evoked Potential (BAEPs) show a flat layout, without wave V, meaning a severe damage of cochlear nerve. A MRI (Siemens Avento 1,5Tesla) has already been realized with 3D Ciss, T1EG sequences with and without gadolinium injection and a TOF sequence. The MRI shows duplicity of cisternal portion of the left trigeminal with a upper bundle emerging from the middle of the pons, at the lateral surface of the brainstem. The lower bundle has an aberrant origin between pons and brainstem at the same level of the acousticofacial nerve bundle. Moreover, it compresse the cochleovestibular nerve from its origin, realising a nervous conflict (figure 1 and 2). TOF et 3DT1 weighted sequences after injection erase the vascular origin of this abnormalities
(figure 3). No vestibulocochlear nerve tumor was noted. The contralateral trigeminal nerve has a modal disposition. The signal of ear inner fluid and vestibular aqueduct fluid are normal.
Discussion
Variations of birth or cranial nerves directions are extremely rare anatomic situations. The trigeminal nerve is a mixte nerve with a sensory nucleus spreaded from the midbrain to the medulla in the general sensory column located laterally. Its motor nulei is located in the branchial motor column, which is shared with the other branchial motor nuclei in particular the VII [1]. In its modal position, the trigeminal nerve emerge from the antero-lateral side of pons at the upper and medium third junction by 2 roots: the largest sensory root and medium then lower one. The two roots cross the pontine cisterne in a vertical and lateral way to the Meckel’s cave [2,3]. There are aberrant or incidental radicels emerging separately from the main sensory root at the antero-lateral side of the pons in half cases [4]. This situation explains the persistence of sensitivity after rhizotomy of the main sensory root of trigeminal nerve [5]. Theses incidental radicels meet the sensory root in its first centimeter after its emergency in 90% cases. The driving root is composed by 7 to 8 radicels on average, born separately and that meets usually at 1 cm from the pons. Incidentals sensory fibers are closer to the sensory root than the motor root [4,5,6].
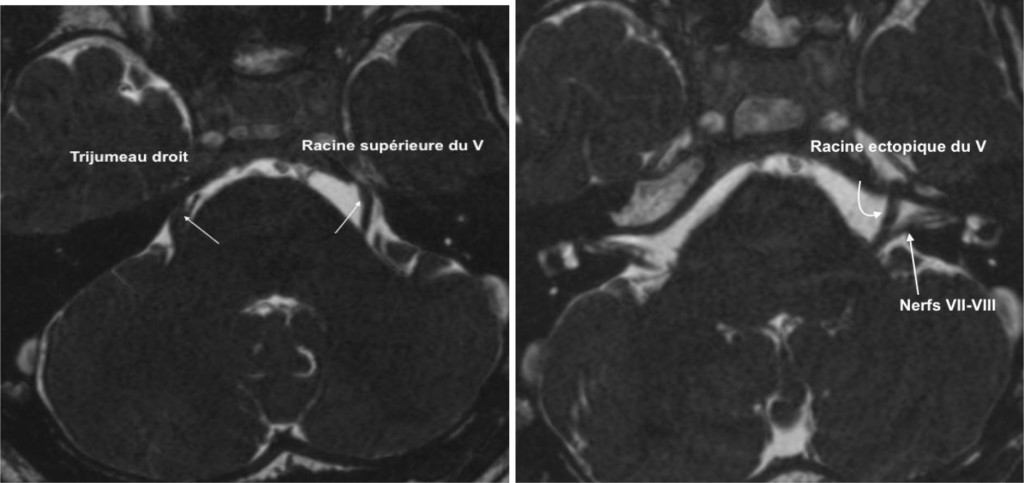
Fig S1. 3D MRI Ciss, axial MinIP. Double emergence of the left trigeminal nerve.
The upper beam with normal emergence at the anterolateral side of the pons (a). The inferior beam with an aberrant origin at the level between the pons and the medulla, pushing back the vestibulocochlear nerve at his origin.
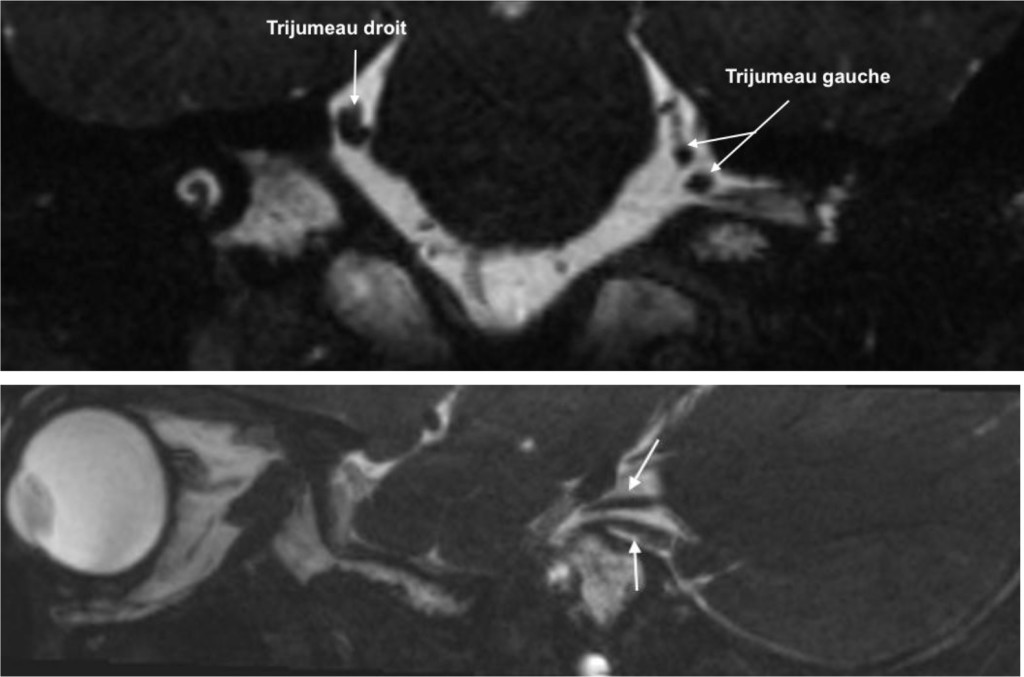
Fig. S2. MRI 3D Ciss reconstruction coronal (a) and sagittal (b). Illustration of the 2 beams of the left trigeminal (double arrow). Modal anatomy of the right trigeminal (arrow).
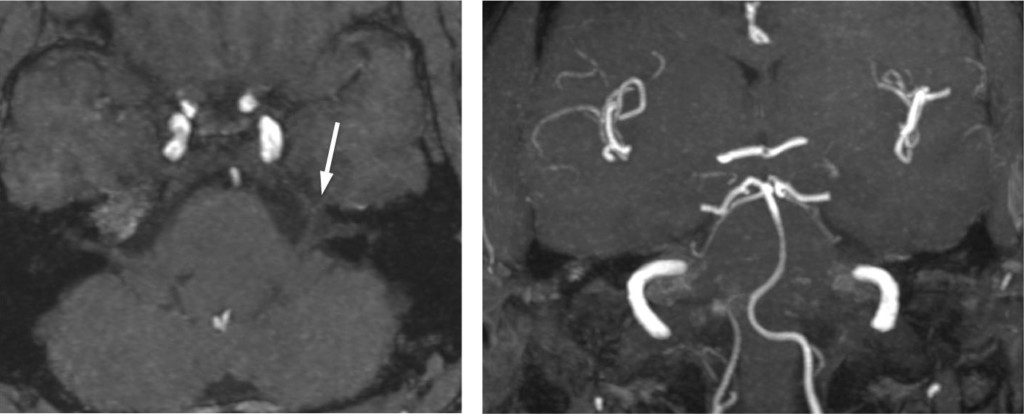
Fig. S3. IRM TOF MPR axial (a) and coronaleT1 (b) with injection eliminate vascular origin.
If duplicity of trigeminal nerve are reports in the anatomical study [4], they have never been described in imaging literature to our knowledge. The other particularity of our case is that aberrant emergency from of one bundles, at the same level of the acousticofacial nerve.
The aberrant bundle, probably the motor root of V, whose the original nucleus is located in the same column than the facial nerve (branchial motor column) explaining the emergency at the same level of the acousticofacial nerve bundle. The compression of cochlear nerve by motor fibers of the trijumeau would explain sensorineural hearing loss observed on the patient. Conflicts at cerebellopontine angle concern the most often Anterior Inferior Cerebellar Artery (AICA) and the acousticofacial nerve bundle or the trigeminal nerve. A conflict between two nervous structures is a rare situation. It very likely that the conflict is the cause of the hearing loss due to the presence of a mass effect on the vestibulocochlear nerve and the absence of other abnormalities that could explain the symptomatology.
Conclusion
Emergence anomalies of cranial nerves on the brainstem are rare. In our knowledge this would be the first case of trigeminal nerve duplicity described in the imaging literature.
References
- Kahle W (2007) Anatomie, Tome 3 Système nerveux et organes des sens – Flammarion Médecine-Sciences: 423.
- Wilson-Pawels, Akeson, Stewart. Cranial nerves: anatomy and clinical comments. Toronto, Philadephia: B.C. Decker Inc.; 1998.
- Leblanc A. Encephalo-peripheral nervous system-vascularization, anatomy, imaging. Berlin, Heidelberg, New York: Springer-Verlag; 2001, 79–210, Trigeminal nerve.
- Gudmundsson K, Rhoton AL Jr, Rushton JG (1971) Detailed anatomy of the intracranial portion of the trigeminal nerve. J Neurosurg 35: 592–600. [crossref]
- Dandy WE (1929) An operation for the cure of tic douloureux: partial section of the sensory root at the pons. Arch Surg 18: 687–734.
- Jannetta PJ, Rand RW (1966) Microanatomy of thetrigeminal nerve. Anat Rec 154: 362.